

Association of primary care characteristics with variations in mortality rates in England: an observational study
- PMID: 23110102
- PMCID: PMC3480536
- DOI: 10.1371/journal.pone.0047800
Association of primary care characteristics with variations in mortality rates in England: an observational study
Abstract
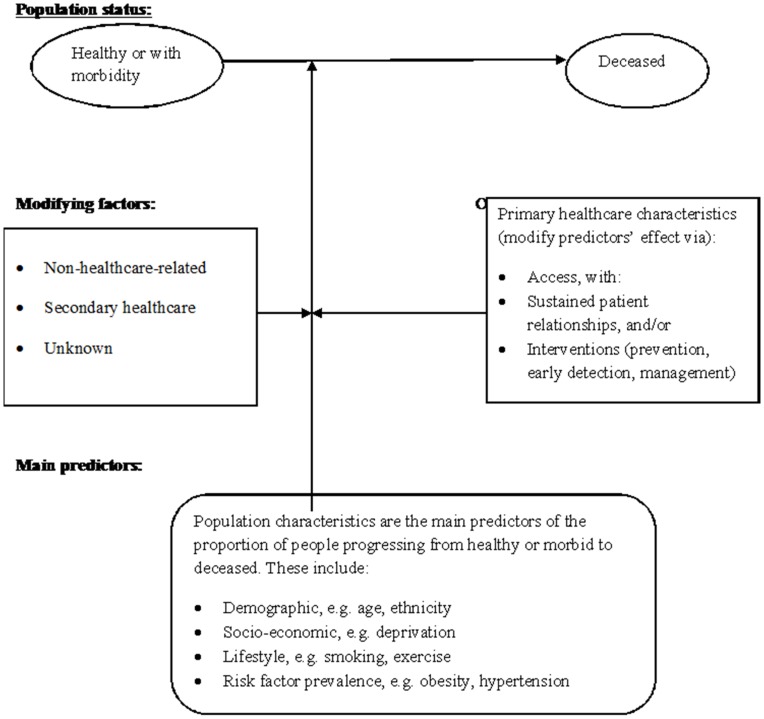
Background: Wide variations in mortality rates persist between different areas in England, despite an overall steady decline. To evaluate a conceptual model that might explain how population and service characteristics influence population mortality variations, an overall null hypothesis was tested: variations in primary healthcare service do not predict variations in mortality at population level, after adjusting for population characteristics.
Methodology/principal findings: In an observational study of all 152 English primary care trusts (geographical groupings of population and primary care services, total population 52 million), routinely available published data from 2008 and 2009 were modelled using negative binomial regression. Counts for all-cause, coronary heart disease, all cancers, stroke, and chronic obstructive pulmonary disease mortality were analyzed using explanatory variables of relevant population and service-related characteristics, including an age-correction factor. The main predictors of mortality variations were population characteristics, especially age and socio-economic deprivation. For the service characteristics, a 1% increase in the percentage of patients on a primary care hypertension register was associated with decreases in coronary heart disease mortality of 3% (95% CI 1-4%, p = 0.006) and in stroke mortality of 6% (CI 3-9%, p<0.0001); a 1% increase in the percentage of patients recalling being better able to see their preferred doctor was associated with decreases in chronic obstructive pulmonary disease mortality of 0.7% (CI 0.2-2.0%, p = 0.02) and in all cancer mortality of 0.3% (CI 0.1-0.5%, p = 0.009) (continuity of care). The study found no evidence of an association at primary care trust population level between variations in achievement of pay for performance and mortality.
Conclusions/significance: Some primary healthcare service characteristics were also associated with variations in mortality at population level, supporting the conceptual model. Health care system reforms should strengthen these characteristics by delivering cost-effective evidence-based interventions to whole populations, and fostering sustained patient-provider partnerships.
Conflict of interest statement
Figures
References
-
- World Health Organisation. Global Health Observatory Data Repository (updated 2011) Noncommunicable diseases. Mortality, All NCDs, deaths per 100,000 (age-standardized estimate) Available: http://apps.who.int/ghodatai/?vd=2490. Accessed 2011 Jul 30.
-
- National Centre for Health Outcomes Development (NCHOD) managed by The NHS Information Centre for health and social care (2011) Available: http://www.nchod.nhs.uk/.Accessed 2011 Jul 22.
-
- Schoen C, Osborn R, Squires D, Doty M, Pierson R, et al.. (2011) New 2011 survey of patients with complex care needs in eleven countries finds that care is often poorly coordinated. Health Affairs (doi: 10.1377/hlthaff.2011.0923). - PubMed
-
- The Marmot Review (2010) Fair society, healthy lives: Strategic review of health inequalities in England post-2010. The Marmot Review: London UK. Available: http://www.instituteofhealthequity.org/Content/FileManager/pdf/fairsocie.... Accessed 2011 Dec 3.
-
- Surgeon General (1964) Smoking and health. Report of the Advisory Committee to the Surgeon General of the Public Health Service. Washington, DC: US Government Printing Office.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
