

Early childhood growth failure and the developmental origins of adult disease: do enteric infections and malnutrition increase risk for the metabolic syndrome?
- PMID: 23110643
- PMCID: PMC3493112
- DOI: 10.1111/j.1753-4887.2012.00543.x
Early childhood growth failure and the developmental origins of adult disease: do enteric infections and malnutrition increase risk for the metabolic syndrome?
Abstract
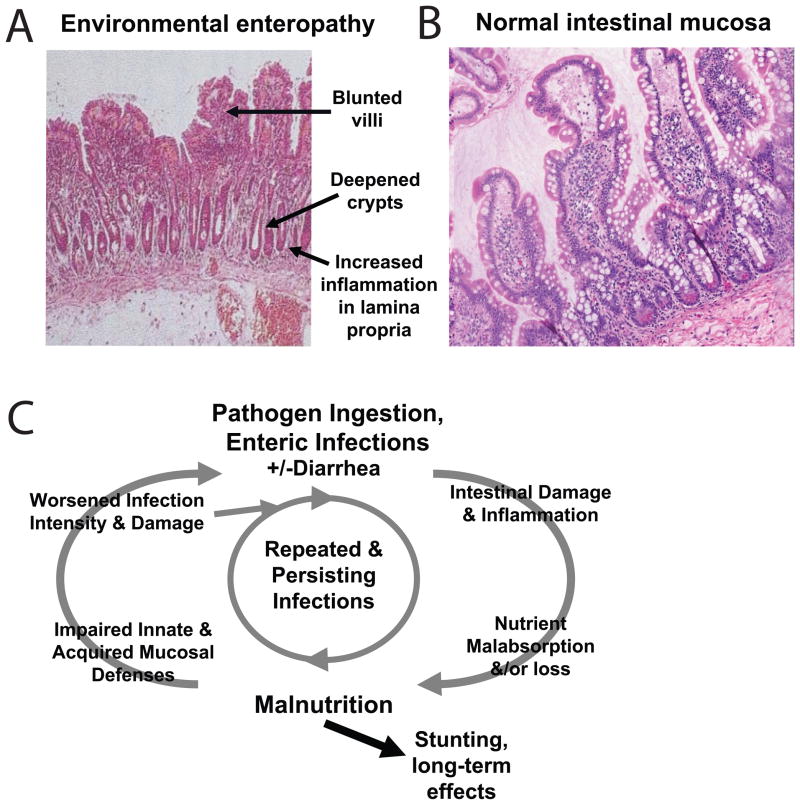
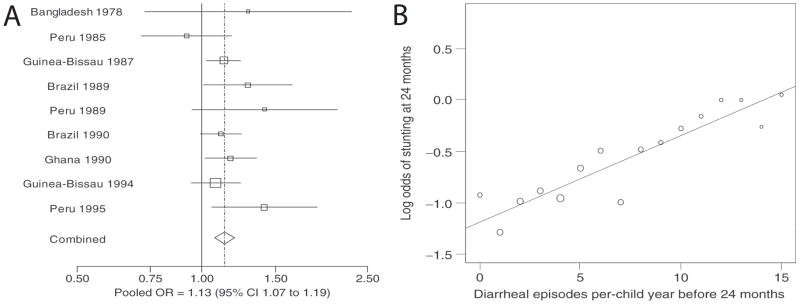
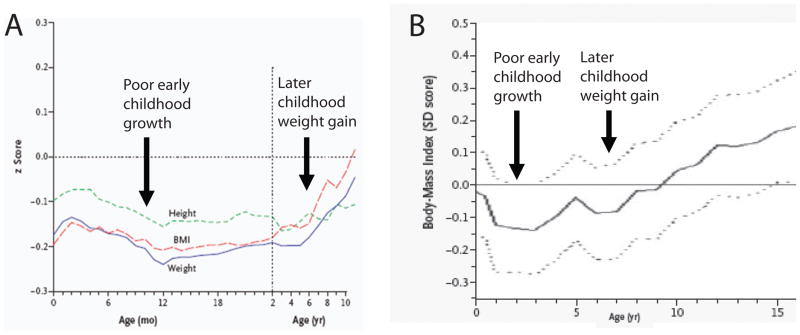
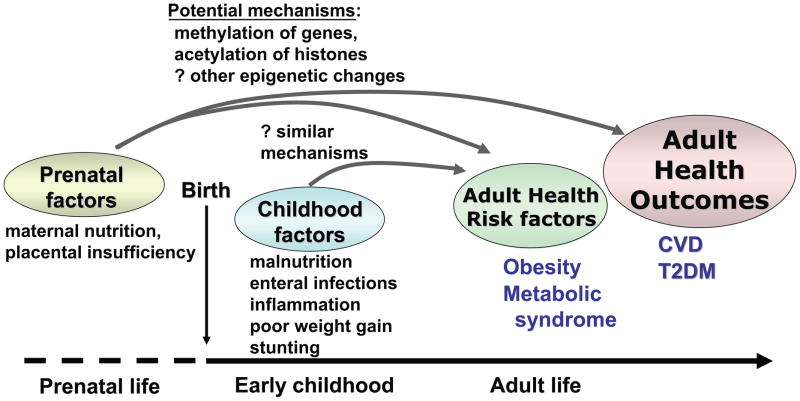
Hypotheses regarding the developmental origins of health and disease postulate that developing fetuses - and potentially young children - undergo adaptive epigenetic changes that have longstanding effects on metabolism and other processes. Ongoing research explores whether these adaptations occur during early life following early childhood malnutrition. In the developing world, there remains a high degree of nutritional stunting, defined as linear growth failure caused by inadequate caloric intake, which may be exacerbated by inflammation from ongoing infections. In areas with poor sanitation, children experience vicious cycles of enteric infections and malnutrition, resulting in poor nutrient absorption as a result of changes in the intestinal mucosa, now termed "environmental enteropathy." Emerging evidence links early childhood diarrhea and/or growth failure with an increased occurrence of risk factors for cardiovascular disease in later life, including dyslipidemia, hypertension, and glucose intolerance. The mechanisms for these associations remain poorly understood and may relate to epigenetic responses to poor nutrition, increased inflammation, or both. Given the increased incidence of cardiovascular disease in developing areas of the world, associations between childhood malnutrition, early-life infections, and the increased occurrence of risk factors for cardiovascular disease underscore further reasons to improve nutrition and infection-related outcomes for young children worldwide.
© 2012 International Life Sciences Institute.
Figures
References
-
- Barker DJ. Fetal programming of coronary heart disease. Trends Endocrinol Metab. 2002 Nov;13(9):364–368. - PubMed
-
- Barker DJ. Adult consequences of fetal growth restriction. Clin Obstet Gynecol. 2006 Jun;49(2):270–283. - PubMed
-
- Bavdekar A, Yajnik CS, Fall CH, et al. Insulin resistance syndrome in 8-year-old Indian children: small at birth, big at 8 years, or both? Diabetes. 1999 Dec;48(12):2422–2429. - PubMed
-
- Veening MA, Van Weissenbruch MM, Delemarre-Van De Waal HA. Glucose tolerance, insulin sensitivity, and insulin secretion in children born small for gestational age. J Clin Endocrinol Metab. 2002 Oct;87(10):4657–4661. - PubMed
-
- Barker DJ, Hales CN, Fall CH, Osmond C, Phipps K, Clark PM. Type 2 (non-insulin-dependent) diabetes mellitus, hypertension and hyperlipidaemia (syndrome X): relation to reduced fetal growth. Diabetologia. 1993 Jan;36(1):62–67. - PubMed
