

Lymphangioleiomyomatosis - a wolf in sheep's clothing
- PMID: 23114603
- PMCID: PMC3484429
- DOI: 10.1172/JCI58709
Lymphangioleiomyomatosis - a wolf in sheep's clothing
Abstract
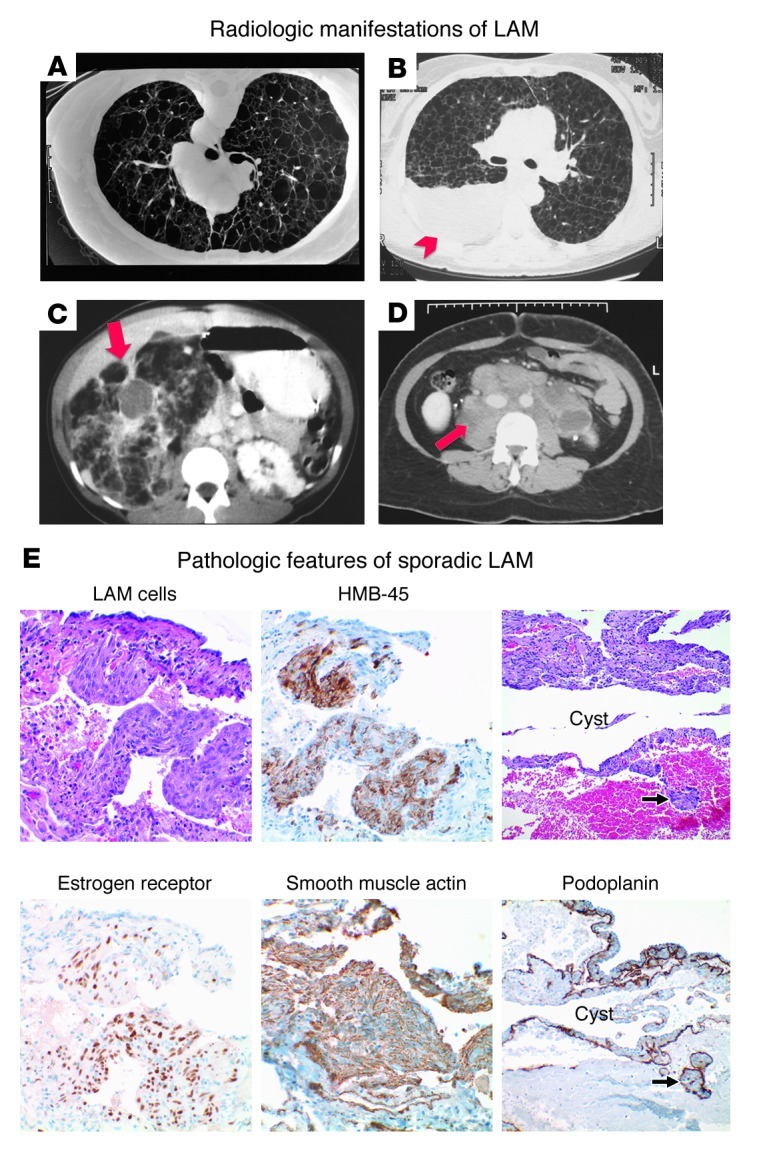
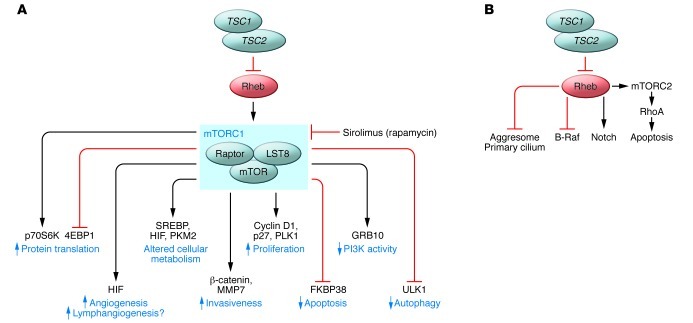
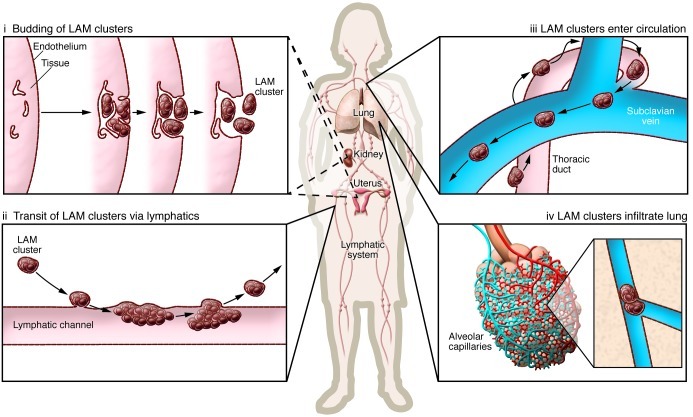
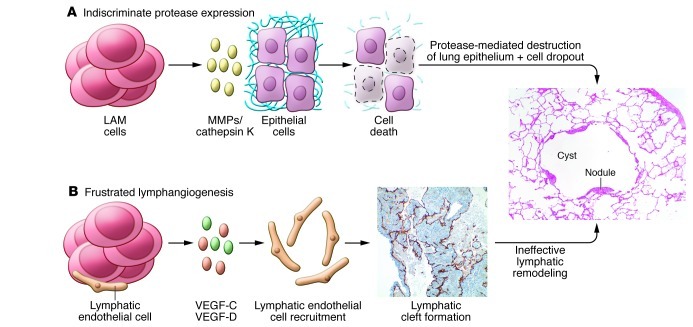
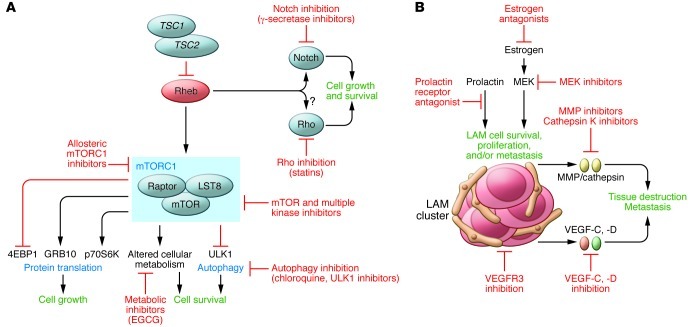
Lymphangioleiomyomatosis (LAM) is a rare progressive lung disease of women. LAM is caused by mutations in the tuberous sclerosis genes, resulting in activation of the mTOR complex 1 signaling network. Over the past 11 years, there has been remarkable progress in the understanding of LAM and rapid translation of this knowledge to an effective therapy. LAM pathogenic mechanisms mirror those of many forms of human cancer, including mutation, metabolic reprogramming, inappropriate growth and survival, metastasis via blood and lymphatic circulation, infiltration/invasion, sex steroid sensitivity, and local and remote tissue destruction. However, the smooth muscle cell that metastasizes, infiltrates, and destroys the lung in LAM arises from an unknown source and has an innocent histological appearance, with little evidence of proliferation. Thus, LAM is as an elegant, monogenic model of neoplasia, defying categorization as either benign or malignant.
Figures
References
-
- Kitaichi M, Nishimura K, Itoh H, Izumi T. Pulmonary lymphangioleiomyomatosis: a report of 46 patients including a clinicopathologic study of prognostic factors. Am J Respir Crit Care Med. 1995;151(2 pt 1):527–533. - PubMed
-
- Johnson SR. Lymphangioleiomyomatosis. Eur Respir J. 2006;27(5):1056–1065. - PubMed
-
- Taveira-DaSilva AM, Steagall WK, Moss J. Lymphangioleiomyomatosis. Cancer Control. 2006;13(4):276–285. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
