

Review
doi: 10.1172/JCI64124.
Epub 2012 Nov 1.
Advances in stem cell therapy for spinal cord injury
Affiliations
- PMID: 23114605
- PMCID: PMC3484454
- DOI: 10.1172/JCI64124
Item in Clipboard
Review
Advances in stem cell therapy for spinal cord injury
J Clin Invest.
2012 Nov.
Abstract
Spinal cord injury (SCI) is a devastating condition producing great personal and societal costs and for which there is no effective treatment. Stem cell transplantation is a promising therapeutic strategy, though much preclinical and clinical research work remains. Here, we briefly describe SCI epidemiology, pathophysiology, and experimental and clinical stem cell strategies. Research in stem cell biology and cell reprogramming is rapidly advancing, with the hope of moving stem cell therapy closer to helping people with SCI. We examine issues important for clinical translation and provide a commentary on recent developments, including termination of the first human embryonic stem cell transplantation trial in human SCI.
Figures
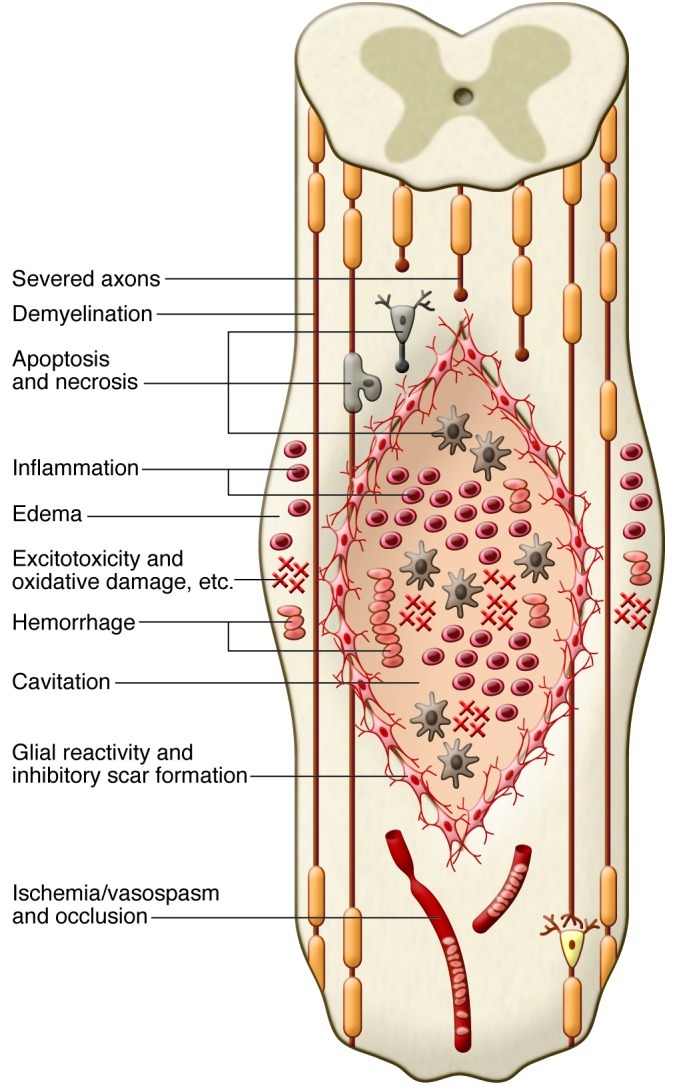
The diagram shows a composite of pathophysiological events occurring after SCI, including the acute (e.g., edema and hemorrhage), subacute (e.g., inflammation), and chronic (e.g., cavitation) phases. The primary and secondary injury mechanisms involve edema, hemorrhage, inflammation, apoptosis, necrosis, excitotoxicity, lipid peroxidation, electrolyte imbalance, ischemia/vasospasm, and blood vessel occlusion. Oligodendrocytes and neurons die, resulting in axonal demyelination and disruption of synaptic transmission. In the subacute and chronic phases, a fluid-filled lentiform-shaped cavity or cyst forms in the center of the cord, with surrounding hypertrophic astrocytes and macrophages. These and other cells secrete extracellular matrix and inhibitory molecules, such as chondroitin sulfate proteoglycans (CSPG), which compose the glial scar, resulting in a physical and chemical barrier to regeneration.
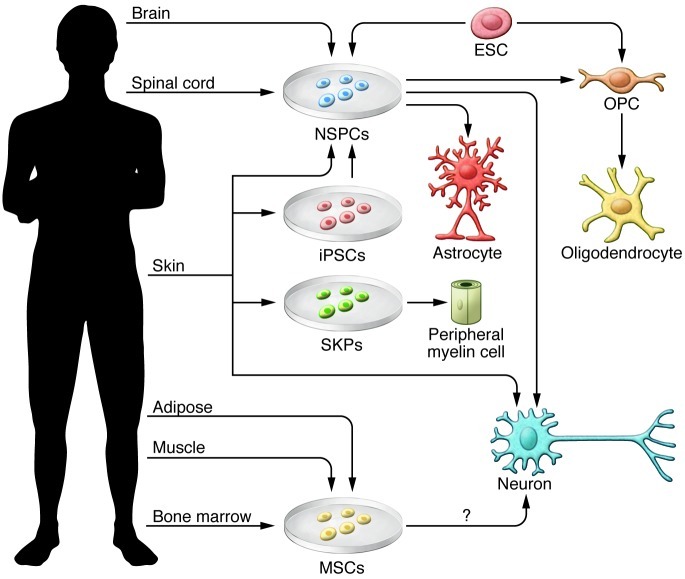
This illustration shows various tissue sources of stem cells, including NSPCs, iPSCs, SKPs, MSCs, ES cells (ESC), and direct conversion methods to yield neural cells for transplantation. NSPCs can be isolated from the fetal and adult brain and spinal cord and differentiated into progenitor cells, such as OPCs and mature oligodendrocytes, or astrocytes or neurons depending on culture conditions and exposure to growth factors. ES cells follow a default pathway to neural cells, and specific conditions can promote OPC generation. MSCs can be derived from a variety of tissues, including BM, umbilical cord, adipose tissue, muscle, and dental pulp from deciduous baby teeth. In culture, MSCs have shown properties of neural cells. Fibroblasts from the skin can be reprogrammed using various methods into iPSCs,which are then directed along a neural lineage. Recent studies have directly converted fibroblasts to neurons and NSPCs, bypassing the pluripotent stage.
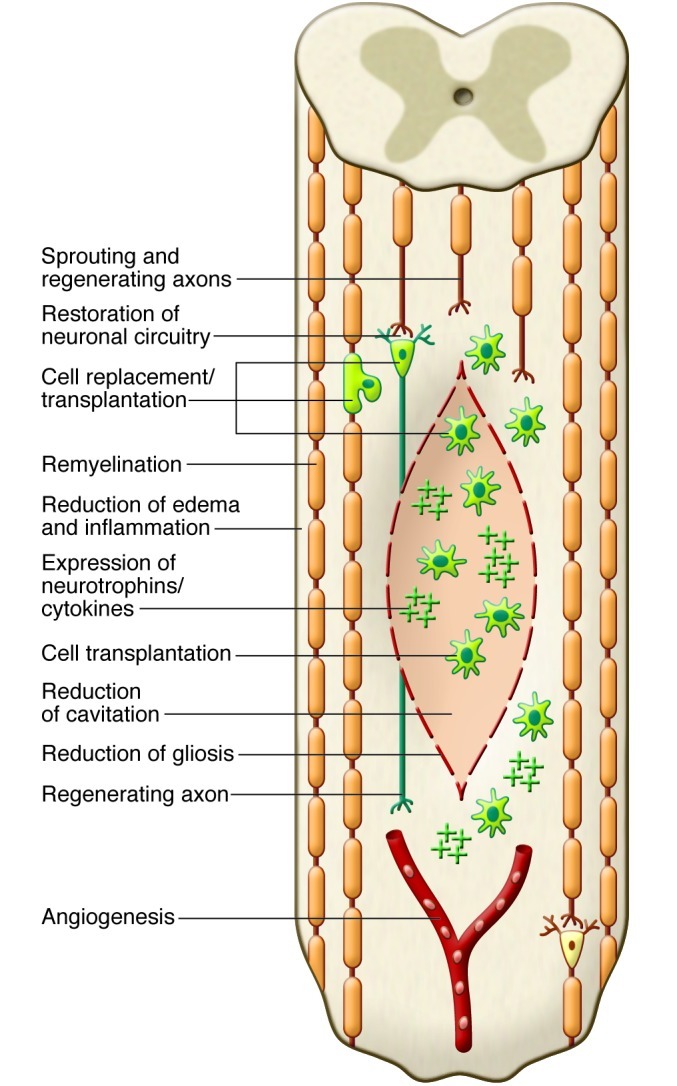
The diagram shows some of the potential mechanisms of repair after transplantation of stem cells into the injured cord. Potential mechanisms include replacement of oligodendrocytes or neurons by transplanted cells (shown in green), remyelination of spared axons, restoration of neuronal circuitry by a new synapse with a transplanted neuron that gives rise to a newly regenerated axon, enhanced preservation of host neuronal and glial cells, for example, by secreted neurotrophins from transplanted cells, promotion of angiogenesis, bridging of the cyst/cavity by transplanted cells, reduction of inflammation or gliosis, stimulation of endogenous precursor cells, and creation of a favorable environment for plasticity and axonal regeneration.
References
-
- Tator CH. Review of treatment trials in human spinal cord injury: issues, difficulties, and recommendations. Neurosurgery. 2006;59(5):957–982. - PubMed
