

Comparison of allogeneic vs autologous bone marrow–derived mesenchymal stem cells delivered by transendocardial injection in patients with ischemic cardiomyopathy: the POSEIDON randomized trial
- PMID: 23117550
- PMCID: PMC4762261
- DOI: 10.1001/jama.2012.25321
Comparison of allogeneic vs autologous bone marrow–derived mesenchymal stem cells delivered by transendocardial injection in patients with ischemic cardiomyopathy: the POSEIDON randomized trial
Erratum in
- JAMA. 2013 Aug 21;310(7):750. George, Richard [added]; Lardo, Albert [added]
Abstract
Context: Mesenchymal stem cells (MSCs) are under evaluation as a therapy for ischemic cardiomyopathy (ICM). Both autologous and allogeneic MSC therapies are possible; however, their safety and efficacy have not been compared.
Objective: To test whether allogeneic MSCs are as safe and effective as autologous MSCs in patients with left ventricular (LV) dysfunction due to ICM.
Design, setting, and patients: A phase 1/2 randomized comparison (POSEIDON study) in a US tertiary-care referral hospital of allogeneic and autologous MSCs in 30 patients with LV dysfunction due to ICM between April 2, 2010, and September 14, 2011, with 13-month follow-up.
Intervention: Twenty million, 100 million, or 200 million cells (5 patients in each cell type per dose level) were delivered by transendocardial stem cell injection into 10 LV sites.
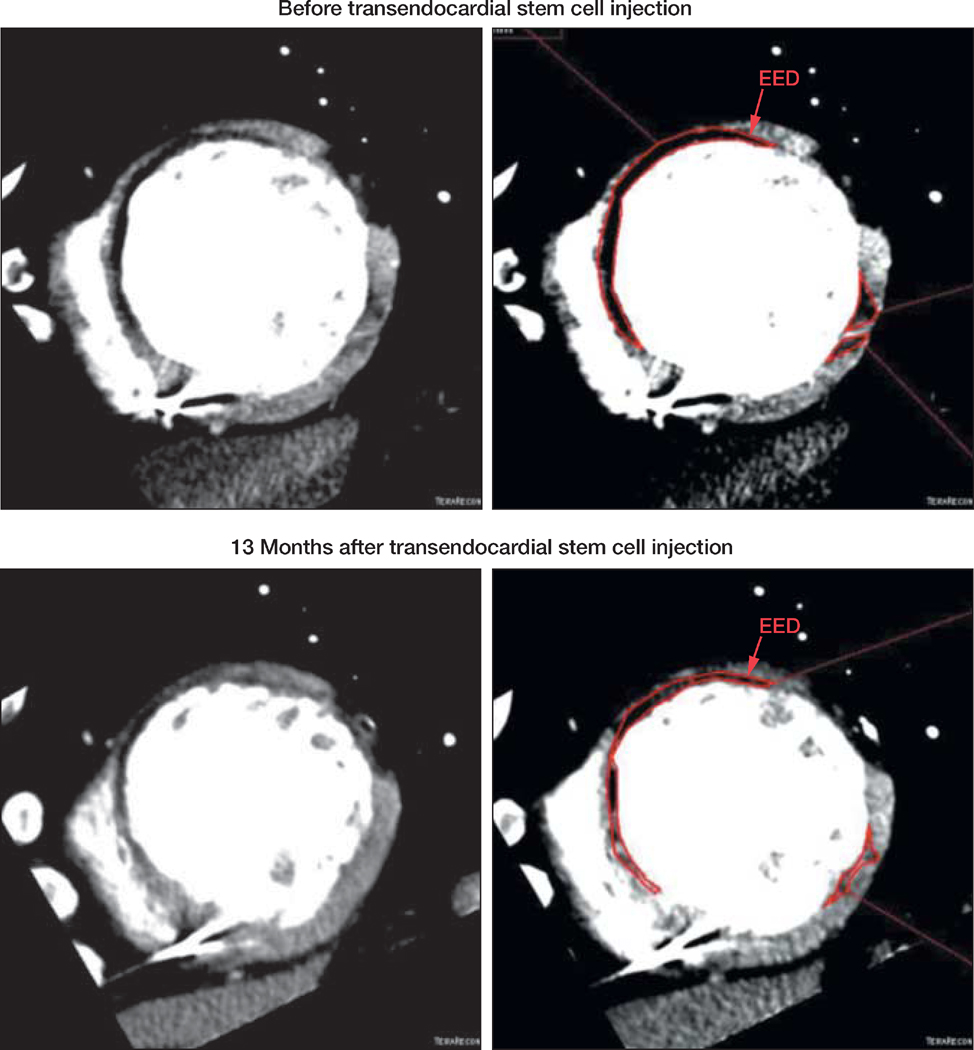
Main outcome measures: Thirty-day postcatheterization incidence of predefined treatment-emergent serious adverse events (SAEs). Efficacy assessments included 6-minute walk test, exercise peak VO2, Minnesota Living with Heart Failure Questionnaire (MLHFQ), New York Heart Association class, LV volumes, ejection fraction (EF), early enhancement defect (EED; infarct size), and sphericity index.
Results: Within 30 days, 1 patient in each group (treatment-emergent SAE rate, 6.7%) was hospitalized for heart failure, less than the prespecified stopping event rate of 25%. The 1-year incidence of SAEs was 33.3% (n = 5) in the allogeneic group and 53.3% (n = 8) in the autologous group (P = .46). At 1 year, there were no ventricular arrhythmia SAEs observed among allogeneic recipients compared with 4 patients (26.7%) in the autologous group (P = .10). Relative to baseline, autologous but not allogeneic MSC therapy was associated with an improvement in the 6-minute walk test and the MLHFQ score, but neither improved exercise VO2 max. Allogeneic and autologous MSCs reduced mean EED by −33.21% (95% CI, −43.61% to −22.81%; P < .001) and sphericity index but did not increase EF. Allogeneic MSCs reduced LV end-diastolic volumes. Low-dose concentration MSCs (20 million cells) produced greatest reductions in LV volumes and increased EF. Allogeneic MSCs did not stimulate significant donor-specific alloimmune reactions.
Conclusions: In this early-stage study of patients with ICM, transendocardial injection of allogeneic and autologous MSCs without a placebo control were both associated with low rates of treatment-emergent SAEs, including immunologic reactions. In aggregate, MSC injection favorably affected patient functional capacity, quality of life, and ventricular remodeling.
Trial registration: clinicaltrials.gov Identifier: NCT01087996.
Conflict of interest statement
Figures



Comment in
-
Mixed results for bone marrow–derived cell therapy for ischemic heart disease.JAMA. 2012 Dec 12;308(22):2405-6. doi: 10.1001/jama.2012.64751. JAMA. 2012. PMID: 23117584 No abstract available.
-
Stem cells. Could it be TIME to abandon BMCs?Nat Rev Cardiol. 2013 Jan;10(1):8. doi: 10.1038/nrcardio.2012.170. Epub 2012 Nov 20. Nat Rev Cardiol. 2013. PMID: 23165067 No abstract available.
-
Use of stem cells for ischemic cardiomyopathy.JAMA. 2013 Apr 10;309(14):1458. doi: 10.1001/jama.2013.2890. JAMA. 2013. PMID: 23571572 No abstract available.
-
Use of stem cells for ischemic cardiomyopathy--reply.JAMA. 2013 Apr 10;309(14):1458-9. doi: 10.1001/jama.2013.2893. JAMA. 2013. PMID: 23571573 No abstract available.
References
-
- Leistner DM, Fischer-Rasokat U, Honold J, et al. Transplantation of progenitor cells and regeneration enhancement in acute myocardial infarction (TOP-CARE-AMI): final 5-year results suggest long-term safety and efficacy. Clin Res Cardiol. 2011;100(10):925–934. - PubMed
-
- Perin EC, Willerson JT, Pepine CJ, et al. Cardiovascular Cell Therapy Research Network (CCTRN) Effect of transendocardial delivery of autologous bone marrow mononuclear cells on functional capacity, left ventricular function, and perfusion in chronic heart failure: the FOCUS-CCTRN trial. JAMA. 2012;307(16):1717–1726. - PMC - PubMed
-
- Schächinger V, Erbs S, Elsässer A, et al. REPAIR-AMI Investigators Intracoronary bone marrow-derived progenitor cells in acute myocardial infarction. N Engl J Med. 2006;355(12):1210–1221. - PubMed
-
- Assmus B, Honold J, Schächinger V, et al. Transcoronary transplantation of progenitor cells after myocardial infarction. N Engl J Med. 2006;355(12):1222–1232. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
