

Can manual ability be measured with a generic ABILHAND scale? A cross-sectional study conducted on six diagnostic groups
- PMID: 23117570
- PMCID: PMC3533037
- DOI: 10.1136/bmjopen-2012-001807
Can manual ability be measured with a generic ABILHAND scale? A cross-sectional study conducted on six diagnostic groups
Abstract
Objectives: Several ABILHAND Rasch-built manual ability scales were previously developed for chronic stroke (CS), cerebral palsy (CP), rheumatoid arthritis (RA), systemic sclerosis (SSc) and neuromuscular disorders (NMD). The present study aimed to explore the applicability of a generic manual ability scale unbiased by diagnosis and to study the nature of manual ability across diagnoses.
Design: Cross-sectional study.
Setting: Outpatient clinic homes (CS, CP, RA), specialised centres (CP), reference centres (CP, NMD) and university hospitals (SSc).
Participants: 762 patients from six diagnostic groups: 103 CS adults, 113 CP children, 112 RA adults, 156 SSc adults, 124 NMD children and 124 NMD adults.
Primary and secondary outcome measures: Manual ability as measured by the ABILHAND disease-specific questionnaires, diagnosis and nature (ie, uni-manual or bi-manual involvement and proximal or distal joints involvement) of the ABILHAND manual activities.
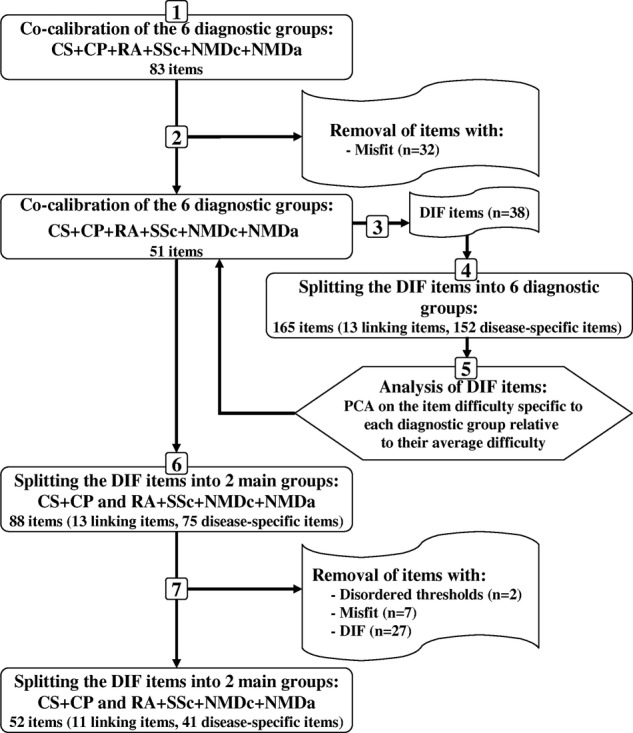
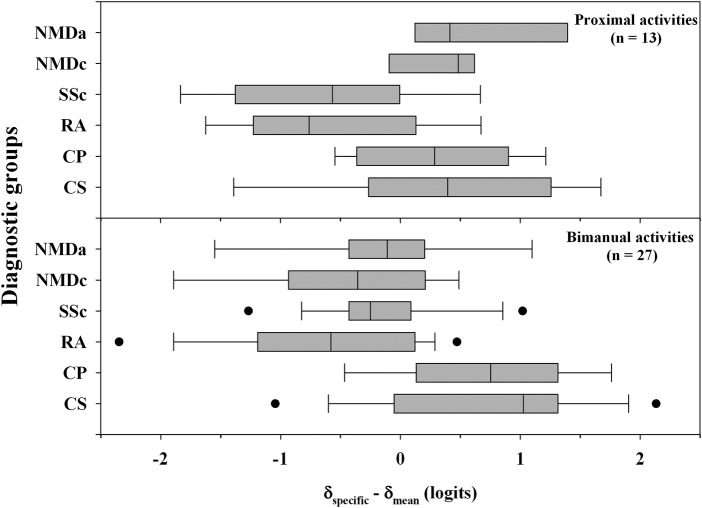
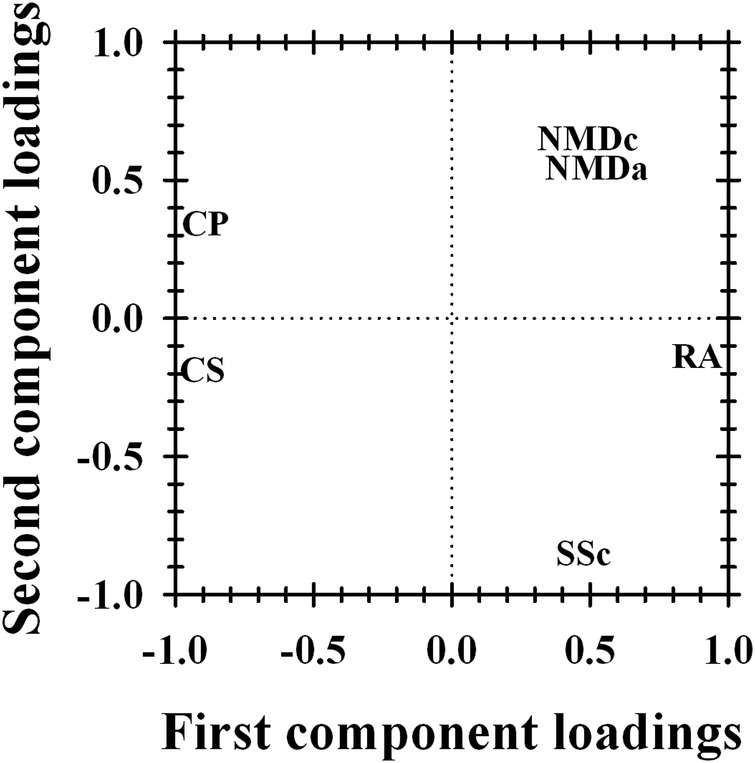
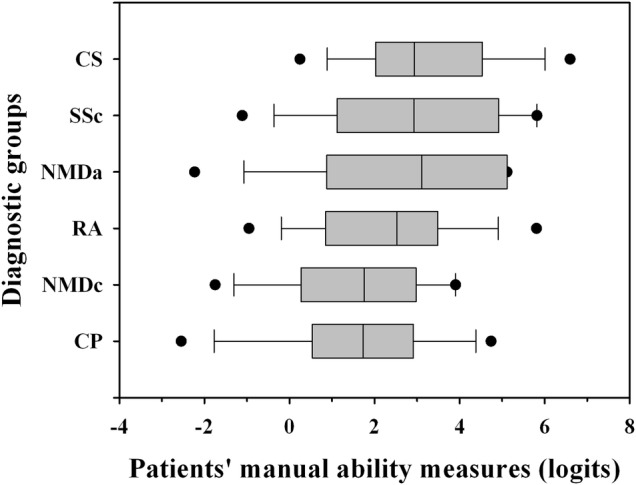
Results: The difficulties of most manual activities were diagnosis dependent. A principal component analysis highlighted that 57% of the variance in the item difficulty between diagnoses was explained by the symmetric or asymmetric nature of the disorders. A generic scale was constructed, from a metric point of view, with 11 items sharing a common difficulty among diagnoses and 41 items displaying a category-specific location (asymmetric: CS, CP; and symmetric: RA, SSc, NMD). This generic scale showed that CP and NMD children had significantly less manual ability than RA patients, who had significantly less manual ability than CS, SSc and NMD adults. However, the generic scale was less discriminative and responsive to small deficits than disease-specific instruments.
Conclusions: Our finding that most of the manual item difficulties were disease-dependent emphasises the danger of using generic scales without prior investigation of item invariance across diagnostic groups. Nevertheless, a generic manual ability scale could be developed by adjusting and accounting for activities perceived differently in various disorders.
Figures
References
-
- Cardol M, de Jong BA, van den Bos GA, et al. Beyond disability: perceived participation in people with a chronic disabling condition. Clin Rehabil 2002;16:27–35 - PubMed
-
- Grimby G, Tennant A, Tesio L. The use of raw scores from ordinal scales: time to end malpractice? J Rehabil Med 2012;44:97–8 - PubMed
-
- Merbitz C, Morris J, Grip JC. Ordinal scales and foundations of misinference. Arch Phys Med Rehabil 1989;70:308–12 - PubMed
-
- Wright BD, Linacre JM. Observations are always ordinal; measurement, however, must be interval. Arch Phys Med Rehabil 1989;70:857–60 - PubMed
-
- Rasch G. Probabilistic models for some intelligence and attainment tests. Chicago: Mesa Press, 1980
LinkOut - more resources
Full Text Sources
Miscellaneous