

Tolvaptan in patients with autosomal dominant polycystic kidney disease
- PMID: 23121377
- PMCID: PMC3760207
- DOI: 10.1056/NEJMoa1205511
Tolvaptan in patients with autosomal dominant polycystic kidney disease
Abstract
Background: The course of autosomal dominant polycystic kidney disease (ADPKD) is often associated with pain, hypertension, and kidney failure. Preclinical studies indicated that vasopressin V(2)-receptor antagonists inhibit cyst growth and slow the decline of kidney function.
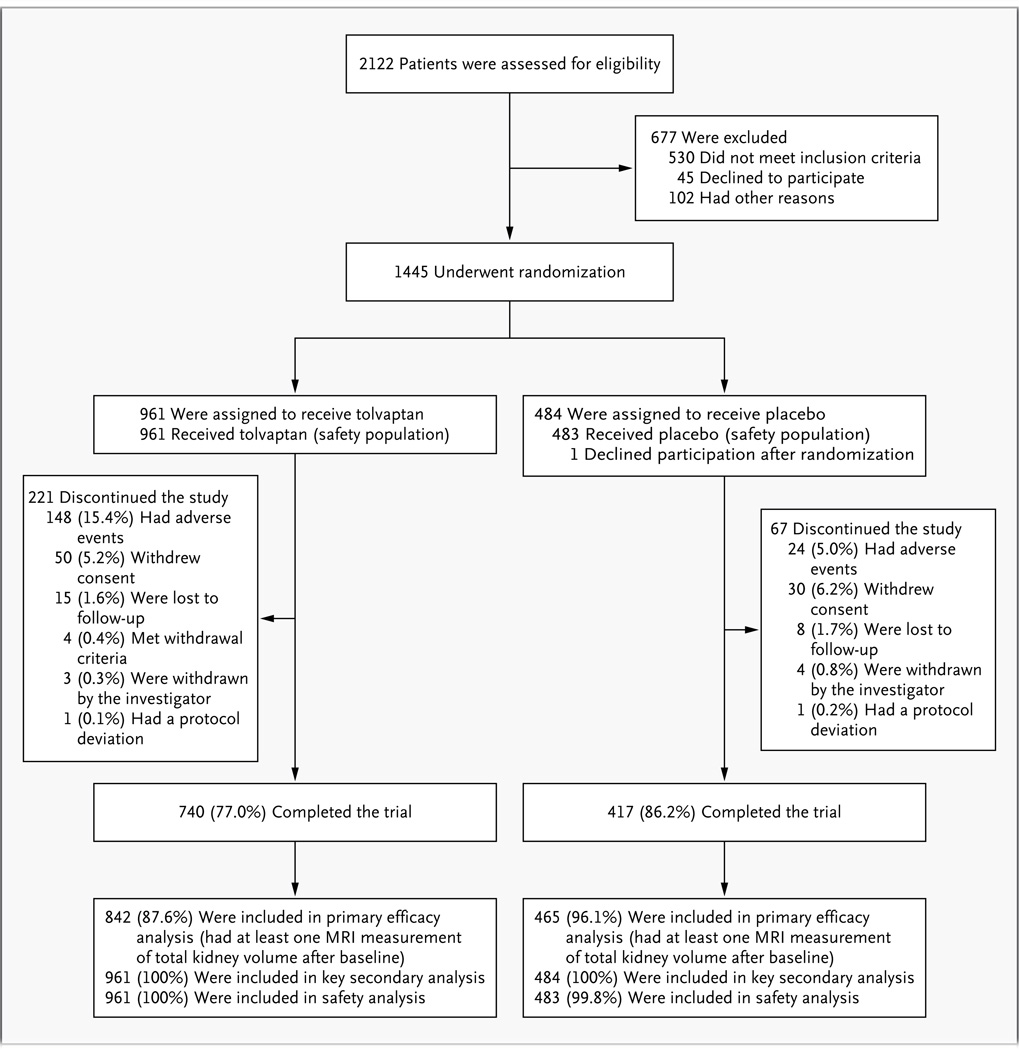
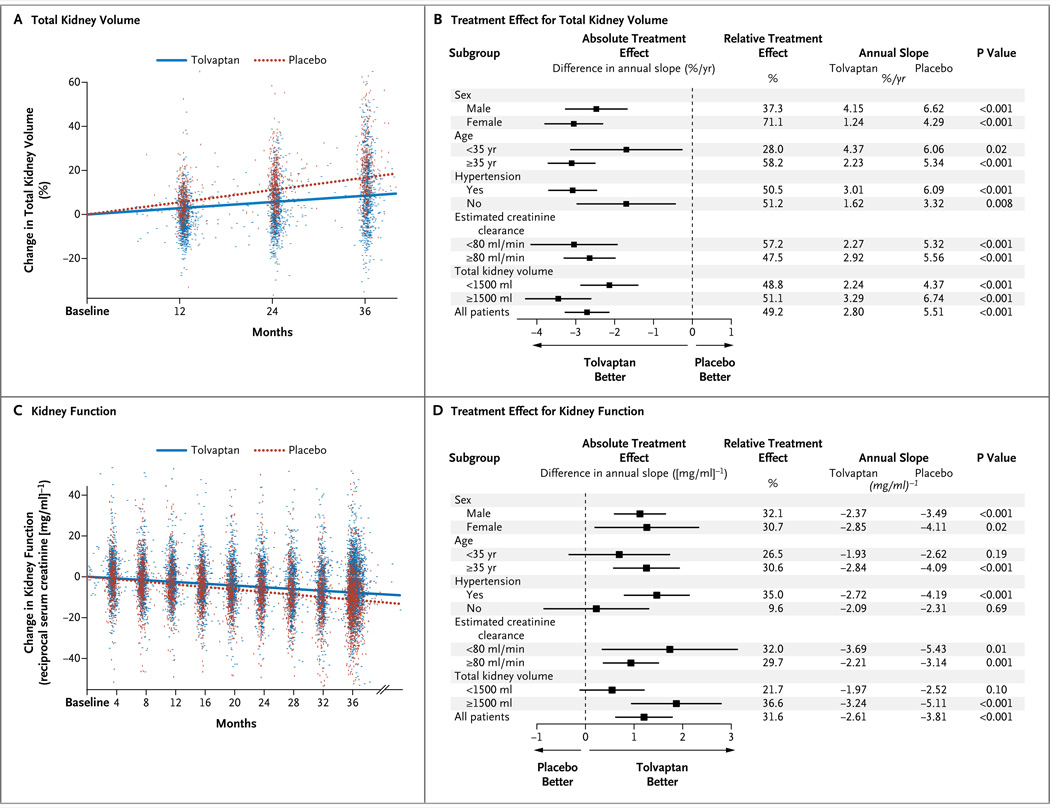
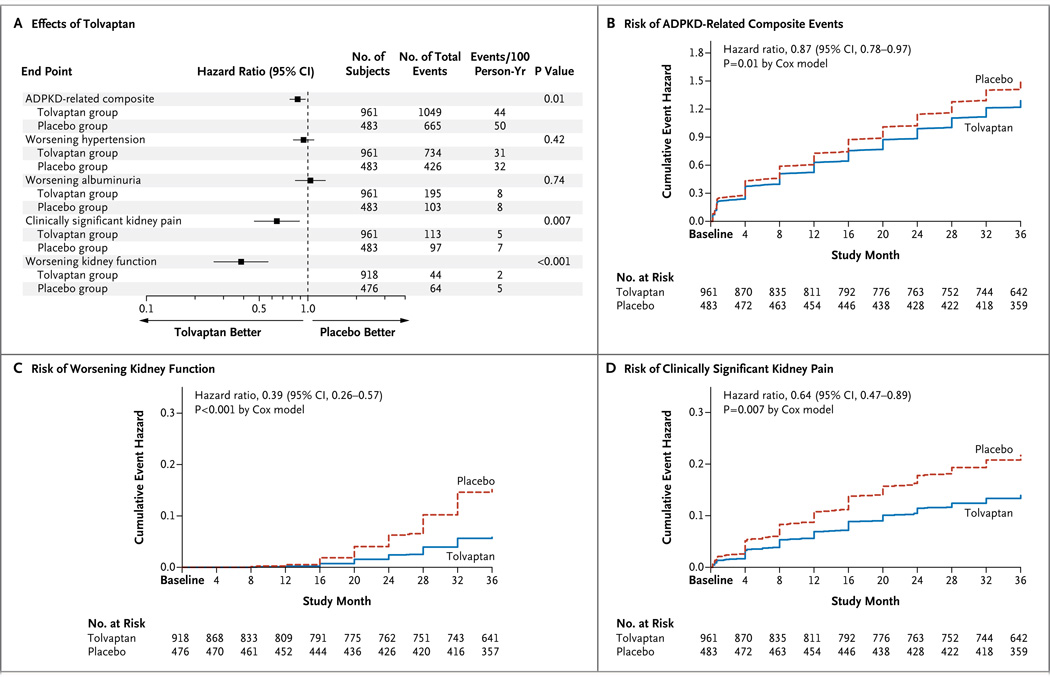
Methods: In this phase 3, multicenter, double-blind, placebo-controlled, 3-year trial, we randomly assigned 1445 patients, 18 to 50 years of age, who had ADPKD with a total kidney volume of 750 ml or more and an estimated creatinine clearance of 60 ml per minute or more, in a 2:1 ratio to receive tolvaptan, a V(2)-receptor antagonist, at the highest of three twice-daily dose regimens that the patient found tolerable, or placebo. The primary outcome was the annual rate of change in the total kidney volume. Sequential secondary end points included a composite of time to clinical progression (defined as worsening kidney function, kidney pain, hypertension, and albuminuria) and rate of kidney-function decline.
Results: Over a 3-year period, the increase in total kidney volume in the tolvaptan group was 2.8% per year (95% confidence interval [CI], 2.5 to 3.1), versus 5.5% per year in the placebo group (95% CI, 5.1 to 6.0; P<0.001). The composite end point favored tolvaptan over placebo (44 vs. 50 events per 100 follow-up-years, P=0.01), with lower rates of worsening kidney function (2 vs. 5 events per 100 person-years of follow-up, P<0.001) and kidney pain (5 vs. 7 events per 100 person-years of follow-up, P=0.007). Tolvaptan was associated with a slower decline in kidney function (reciprocal of the serum creatinine level, -2.61 [mg per milliliter](-1) per year vs. -3.81 [mg per milliliter](-1) per year; P<0.001). There were fewer ADPKD-related adverse events in the tolvaptan group but more events related to aquaresis (excretion of electrolyte-free water) and hepatic adverse events unrelated to ADPKD, contributing to a higher discontinuation rate (23%, vs. 14% in the placebo group).
Conclusions: Tolvaptan, as compared with placebo, slowed the increase in total kidney volume and the decline in kidney function over a 3-year period in patients with ADPKD but was associated with a higher discontinuation rate, owing to adverse events. (Funded by Otsuka Pharmaceuticals and Otsuka Pharmaceutical Development and Commercialization; TEMPO 3:4 ClinicalTrials.gov number, NCT00428948.).
Figures
Comment in
-
Aquaretic treatment in polycystic kidney disease.N Engl J Med. 2012 Dec 20;367(25):2440-2. doi: 10.1056/NEJMe1211857. Epub 2012 Nov 3. N Engl J Med. 2012. PMID: 23121376 No abstract available.
-
Polycystic kidney disease: Tolvaptan in ADPKD-TEMPO 3:4 trial results.Nat Rev Nephrol. 2013 Jan;9(1):1. doi: 10.1038/nrneph.2012.236. Epub 2012 Nov 27. Nat Rev Nephrol. 2013. PMID: 23183839 No abstract available.
-
Commentary on: Tolvaptan in patients with autosomal-dominant polycystic kidney disease.Urology. 2013 Apr;81(4):705-6. doi: 10.1016/j.urology.2012.12.002. Epub 2013 Jan 30. Urology. 2013. PMID: 23375912 No abstract available.
-
Tolvaptan in autosomal dominant polycystic kidney disease.N Engl J Med. 2013 Mar 28;368(13):1259. doi: 10.1056/NEJMc1300762. N Engl J Med. 2013. PMID: 23534568 No abstract available.
-
Tolvaptan in autosomal dominant polycystic kidney disease.N Engl J Med. 2013 Mar 28;368(13):1257. doi: 10.1056/NEJMc1300762. N Engl J Med. 2013. PMID: 23534569 No abstract available.
-
Tolvaptan in autosomal dominant polycystic kidney disease.N Engl J Med. 2013 Mar 28;368(13):1257-8. doi: 10.1056/NEJMc1300762. N Engl J Med. 2013. PMID: 23534570 No abstract available.
-
Tolvaptan in autosomal dominant polycystic kidney disease.N Engl J Med. 2013 Mar 28;368(13):1258. doi: 10.1056/NEJMc1300762. N Engl J Med. 2013. PMID: 23534571 No abstract available.
-
Tolvaptan in autosomal dominant polycystic kidney disease.N Engl J Med. 2013 Mar 28;368(13):1258-9. doi: 10.1056/NEJMc1300762. N Engl J Med. 2013. PMID: 23534572 No abstract available.
-
Doubts about the efficacy of tolvaptan for polycystic kidney disease.Clin Nephrol. 2020 Jun;93(6):307-309. doi: 10.5414/CN109927Letter. Clin Nephrol. 2020. PMID: 32000887 No abstract available.
-
Reply to Dr. Anderson's letter.Clin Nephrol. 2020 Jun;93(6):310-311. doi: 10.5414/CN109927Reply. Clin Nephrol. 2020. PMID: 32000888 No abstract available.
References
-
- Torres VE, Harris PC, Pirson Y. Autosomal dominant polycystic kidney disease. Lancet. 2007;369:1287–1301. - PubMed
-
- Grantham JJ. Autosomal dominant polycystic kidney disease. N Engl J Med. 2008;359:1477–1485. - PubMed
-
- Gattone VHII, Maser RL, Tian C, Rosenberg JM, Branden MG. Developmental expression of urine concentration‱ associated genes and their altered expression in murine infantile-type polycystic kidney disease. Dev Genet. 1999;24:309–318. - PubMed
-
- Gattone VH, Wang X, Harris PC, Torres VE. Inhibition of renal cystic disease development and progression by a vasopressin V2 receptor antagonist. Nat Med. 2003;9:1323–1326. - PubMed
-
- Torres VE, Wang X, Qian Q, Somlo S, Harris PC, Gattone VHII. Effective treatment of an orthologous model of autosomal dominant polycystic kidney disease. Nat Med. 2004;10:363–364. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical