

Postural tachycardia syndrome: a heterogeneous and multifactorial disorder
- PMID: 23122672
- PMCID: PMC3547546
- DOI: 10.1016/j.mayocp.2012.08.013
Postural tachycardia syndrome: a heterogeneous and multifactorial disorder
Abstract
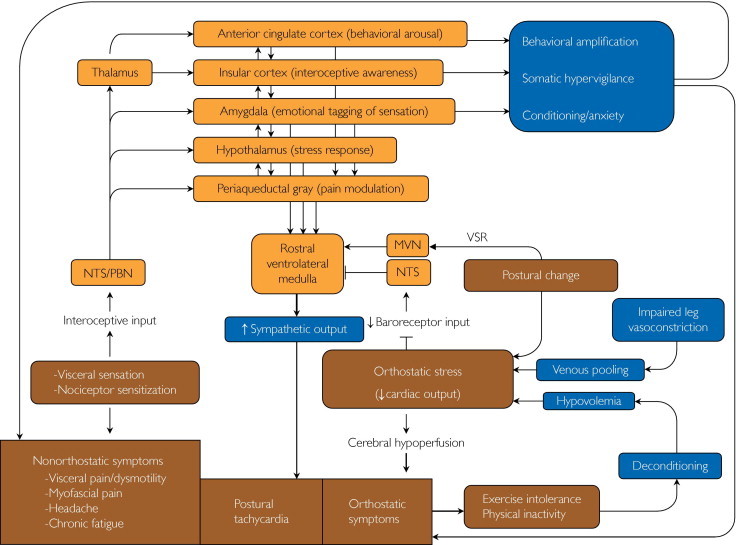
Postural tachycardia syndrome (POTS) is defined by a heart rate increment of 30 beats/min or more within 10 minutes of standing or head-up tilt in the absence of orthostatic hypotension; the standing heart rate is often 120 beats/min or higher. POTS manifests with symptoms of cerebral hypoperfusion and excessive sympathoexcitation. The pathophysiology of POTS is heterogeneous and includes impaired sympathetically mediated vasoconstriction, excessive sympathetic drive, volume dysregulation, and deconditioning. POTS is frequently included in the differential diagnosis of chronic unexplained symptoms, such as inappropriate sinus tachycardia, chronic fatigue, chronic dizziness, or unexplained spells in otherwise healthy young individuals. Many patients with POTS also report symptoms not attributable to orthostatic intolerance, including those of functional gastrointestinal or bladder disorders, chronic headache, fibromyalgia, and sleep disturbances. In many of these cases, cognitive and behavioral factors, somatic hypervigilance associated with anxiety, depression, and behavioral amplification contribute to symptom chronicity. The aims of evaluation in patients with POTS are to exclude cardiac causes of inappropriate tachycardia; elucidate, if possible, the most likely pathophysiologic basis of postural intolerance; assess for the presence of treatable autonomic neuropathies; exclude endocrine causes of a hyperadrenergic state; evaluate for cardiovascular deconditioning; and determine the contribution of emotional and behavioral factors to the patient's symptoms. Management of POTS includes avoidance of precipitating factors, volume expansion, physical countermaneuvers, exercise training, pharmacotherapy (fludrocortisone, midodrine, β-blockers, and/or pyridostigmine), and behavioral-cognitive therapy. A literature search of PubMed for articles published from January 1, 1990, to June 15, 2012, was performed using the following terms (or combination of terms): POTS; postural tachycardia syndrome, orthostatic; orthostatic; syncope; sympathetic; baroreceptors; vestibulosympathetic; hypovolemia; visceral pain; chronic fatigue; deconditioning; headache; Chiari malformation; Ehlers-Danlos; emotion; amygdala; insula; anterior cingulate; periaqueductal gray; fludrocortisone; midodrine; propranolol; β-adrenergic; and pyridostigmine. Studies were limited to those published in English. Other articles were identified from bibliographies of the retrieved articles.
Copyright © 2012 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Low P.A., Opfer-Gehrking T.L., Textor S.C. Postural tachycardia syndrome (POTS) Neurology. 1995;45(4, suppl 5):S19–S25. - PubMed
-
- Freeman R., Wieling W., Axelrod F.B. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Clin Auton Res. 2011;21(2):69–72. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
