

Prognosis of individuals with asymptomatic left ventricular systolic dysfunction in the multi-ethnic study of atherosclerosis (MESA)
- PMID: 23124035
- PMCID: PMC3533250
- DOI: 10.1161/CIRCULATIONAHA.112.112201
Prognosis of individuals with asymptomatic left ventricular systolic dysfunction in the multi-ethnic study of atherosclerosis (MESA)
Abstract
Background: Limited data exist on the prevalence, associations, and prognosis of individuals with asymptomatic left ventricular systolic dysfunction (ALVSD), especially in populations without previous clinical cardiovascular disease (CVD).
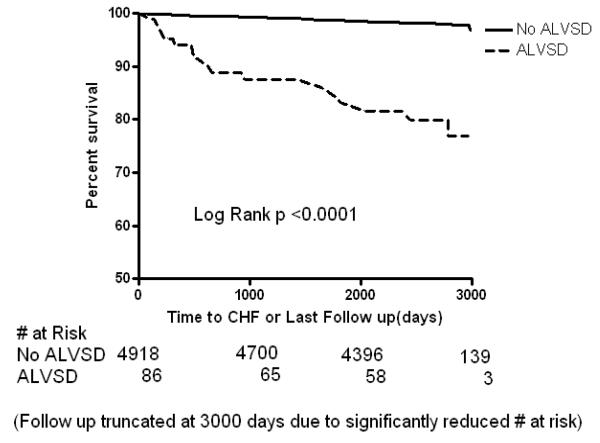
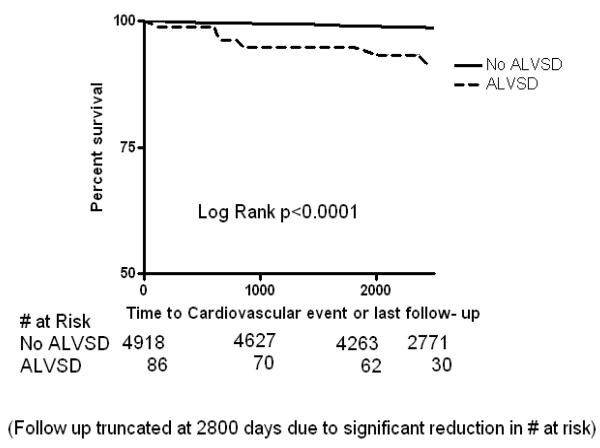
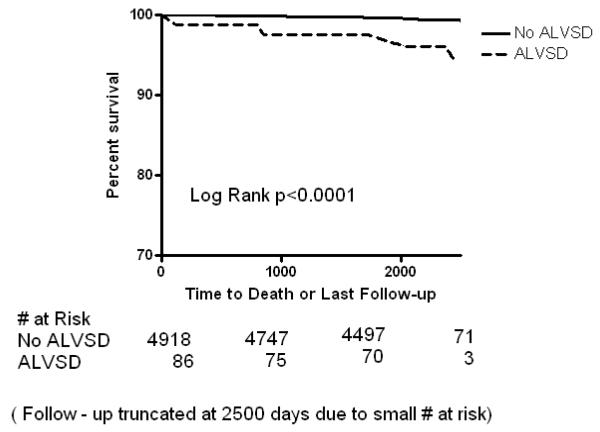
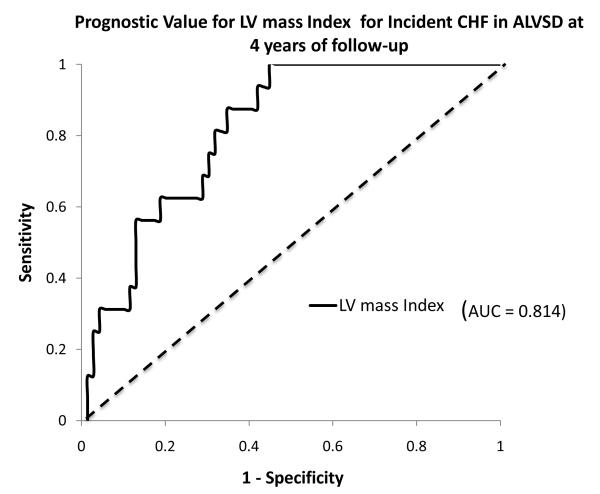
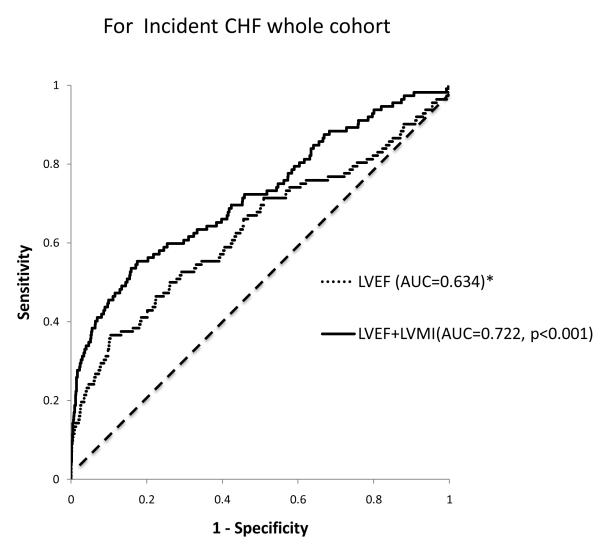
Methods and results: Kaplan-Meier and Cox proportional hazard analyses were used to assess the association between ALVSD, defined as left ventricular ejection fraction <50%, and adjudicated incident congestive heart failure (CHF), all-cause mortality, and CVD events. Of 5004 participants, 112 participants had CHF, 321 had a CVD event, and 278 died after 9 years of follow-up. The overall prevalence of ALVSD was 1.7%, with a higher prevalence in blacks (2.6%). ALVSD had a worse cardiovascular risk profile and was also associated with increased risk in unadjusted and adjusted models for incident CHF (HR [hazard ratio] [95% CI {confidence interval}]: 12.0 [7.04-20.3], P<0.0001 and 8.69 [4.89-15.45], P<0.001 respectively), CVD (HR [95% CI]: 3.32 [1.98-5.58], P<0.001 and 2.21 [1.30-3.73], P=0.003 respectively), and all-cause mortality (HR [95% CI]: 3.47 [2.03-5.94], P<0.0001 and 2.00 [1.13-3.54], P=0.017, respectively). A 10% decrement in left ventricular ejection fraction at baseline was associated with an increase in risk in unadjusted and adjusted models for clinical CHF (HR [95% CI]: 2.17 [1.82-2.63], P<0.0001 and 2.13 [1.73-2.51], P<0.001, respectively) and all-cause mortality (HR [95% CI]: 1.22 [1.05-1.41], P=0.009 and 1.17 [1.00-1.36], P=0.047, respectively). Among the subset of participants with ALVSD, the left ventricular mass index was particularly informative about risk for incident CHF (c-index=0.74).
Conclusions: ALVSD is uncommon in individuals without previous clinical CVD, but it is associated with high risk for CHF, CVD, and all-cause mortality. The left ventricular mass index had good discrimination for incident CHF in Multi-Ethnic Study of Atherosclerosis (MESA) participants with ALVSD.
Figures
References
-
- Levy D, Kenchaiah S, Larson MG, Benjamin EJ, Kupka MJ, Ho KK, Murabito JM, Vasan RS. Long-term trends in the incidence of and survival with heart failure. N Engl J Med. 2002;347:1397–1402. - PubMed
-
- Mann DL. Mechanism and models in heart failure: a combinatorial approach. Circulation. 1999;100:999–1008. - PubMed
-
- Pfeffer MA, Braunwald E. Ventricular remodeling after myocardial infarction: experimental observations and clinical implications. Circulation. 1990;81:1161–172. - PubMed
-
- McMurray JV, McDonagh TA, Davie AP, Cleland JG, Francis CM, Morrison C. Should we screen for asymptomatic left ventricular dysfunction to prevent heart failure. Eur Heart J. 1998;19:842–846. - PubMed
-
- Hunt SA, Baker DW, Chin MH, Cinquegrani MP, Feldman AM, Francis GS, Ganiats TG, Goldstein S, Gregoratos G, Jessup ML, Noble RJ, Packer M, Silver MA, Stevenson LW, Gibbons RJ, Antman EM, Alpert JS, Faxon DP, Fuster V, Jacobs AK, Hiratzka LF, Russell RO, Smith SC, Jr, American College of Cardiology/American Heart Association ACC/AHA guidelines for the evaluation and management of chronic heart failure in the adult: executive summary. A report of the American College of Cardiology /American Heart Association Task Force on practice guidelines. J Am Coll Cardiol. 2001;38:2011–2113. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
