

Association between AKI, recovery of renal function, and long-term outcomes after hospital discharge
- PMID: 23124779
- PMCID: PMC3562863
- DOI: 10.2215/CJN.06480612
Association between AKI, recovery of renal function, and long-term outcomes after hospital discharge
Abstract
Background and objectives: This study aimed to determine if recovery of kidney function after AKI modifies the association between AKI during hospitalization and adverse outcomes after discharge.
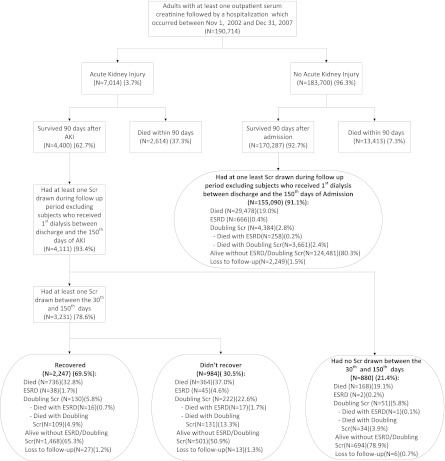
Design, setting, participants, & measurements: The effect of renal recovery after AKI was evaluated in a population-based cohort study (n=190,714) with participants identified from a provincial claims registry in Alberta, Canada, between November 1, 2002 and December 31, 2007. AKI was identified by a two-fold increase between prehospital and peak in-hospital serum creatinine (SCr). Recovery was assessed using SCr drawn closest to 90 days after the AKI event. All-cause mortality and a combined renal outcome of sustained doubling of SCr or progression to kidney failure were evaluated.
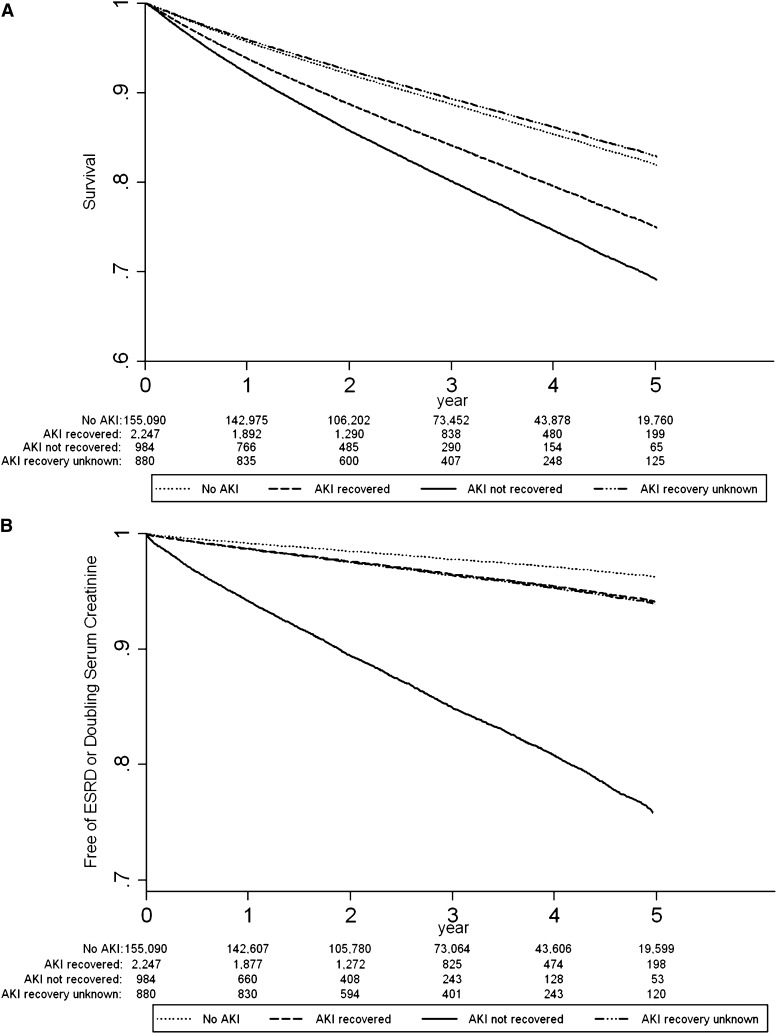
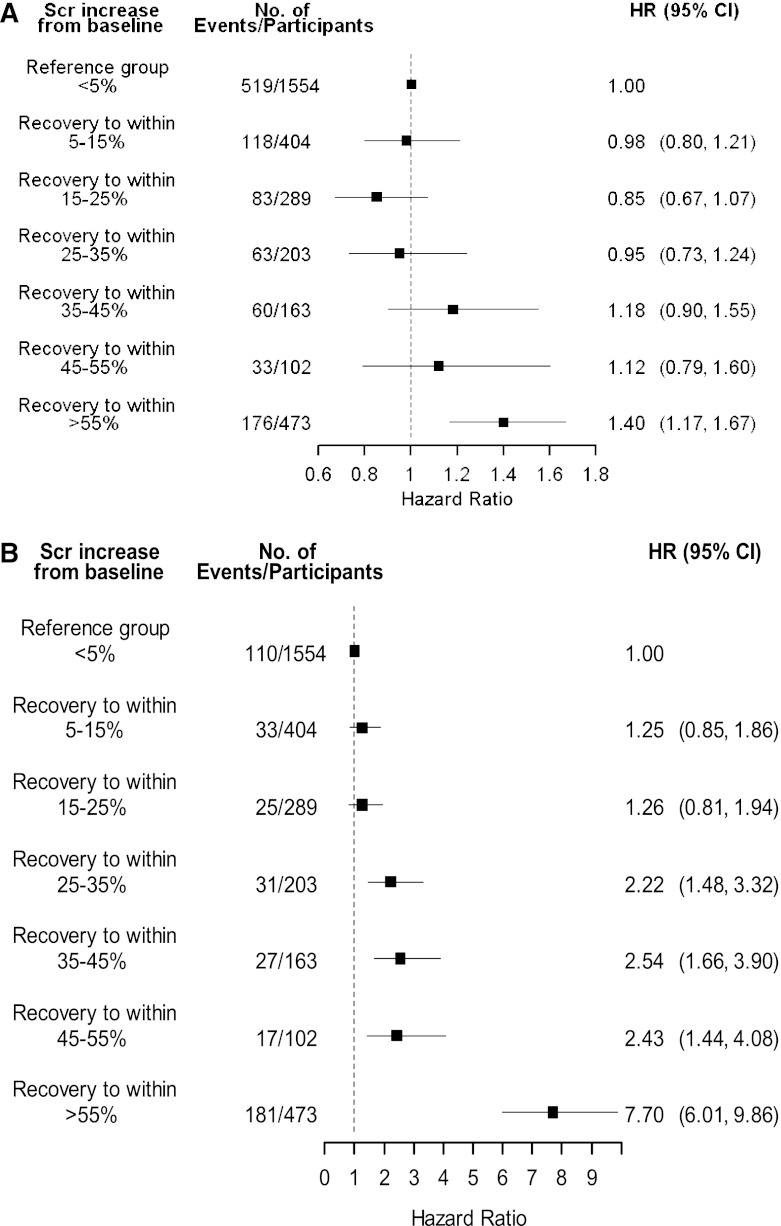
Results: Overall, 3.7% of the participants (n=7014) had AKI, 62.7% of whom (n=4400) survived 90 days. In the 3231 patients in whom recovery could be assessed over a median follow-up of 34 months, 30.8% (n=1268) of AKI survivors died and 2.1% (n=85) progressed to kidney failure. Participants who did not recover kidney function had a higher risk for mortality and adverse renal outcomes when AKI participants who recovered to within 25% of baseline SCr were used as the reference group (adjusted mortality hazard ratio (HR), 1.26; 95% confidence interval, 1.10, 1.43) (adjusted renal outcomes HR, 4.13; 95% confidence interval, 3.38, 5.04). Mortality HR was notably higher when participants failed to recover within 55% of baseline.
Conclusions: Renal recovery after AKI is associated with a lower risk of death or adverse renal outcomes after hospital discharge.
Figures
Comment in
-
Is it AKI or nonrecovery of renal function that is important for long-term outcomes?Clin J Am Soc Nephrol. 2013 Feb;8(2):173-6. doi: 10.2215/CJN.12621212. Epub 2013 Jan 10. Clin J Am Soc Nephrol. 2013. PMID: 23307878 Free PMC article. No abstract available.
References
-
- Levey AS, Atkins R, Coresh J, Cohen EP, Collins AJ, Eckardt KU, Nahas ME, Jaber BL, Jadoul M, Levin A, Powe NR, Rossert J, Wheeler DC, Lameire N, Eknoyan G: Chronic kidney disease as a global public health problem: Approaches and initiatives - a position statement from Kidney Disease Improving Global Outcomes. Kidney Int 72: 247–259, 2007 - PubMed
-
- Tonelli M, Wiebe N, Culleton B, House A, Rabbat C, Fok M, McAlister F, Garg AX: Chronic kidney disease and mortality risk: A systematic review. J Am Soc Nephrol 17: 2034–2047, 2006 - PubMed
-
- Trivedi HS, Pang MM, Campbell A, Saab P: Slowing the progression of chronic renal failure: Economic benefits and patients’ perspectives. Am J Kidney Dis 39: 721–729, 2002 - PubMed
-
- Eknoyan G, Lameire N, Barsoum R, Eckardt KU, Levin A, Levin N, Locatelli F, MacLeod A, Vanholder R, Walker R, Wang H: The burden of kidney disease: Improving global outcomes. Kidney Int 66: 1310–1314, 2004 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
