

Clinical and transcriptional response to the long-acting interleukin-1 blocker canakinumab in Blau syndrome-related uveitis
- PMID: 23124805
- PMCID: PMC3684148
- DOI: 10.1002/art.37776
Clinical and transcriptional response to the long-acting interleukin-1 blocker canakinumab in Blau syndrome-related uveitis
Abstract
Objective: To report on the clinical response to canakinumab in a patient with sporadic nucleotide-binding oligomerization domain-containing protein 2 (NOD-2)-associated pediatric granulomatous arthritis (Blau syndrome) and severe resistant panuveitis, and to describe gene expression profile changes throughout such treatment.
Methods: A 4-year-old boy was diagnosed as having Blau syndrome on the basis of typical clinical features, histologic evidence of noncaseating granulomas, and a NOD2 mutation. Ocular involvement was initially controlled by topical and oral corticosteroids, but over the years visual impairment and complications, such as macular edema and retinal detachment, progressed. Ocular disease remained persistently active despite treatment with multiple different immunosuppressants; therefore, canakinumab treatment was started. Before and during the first 6 months of treatment, the gene expression profile was determined each month.
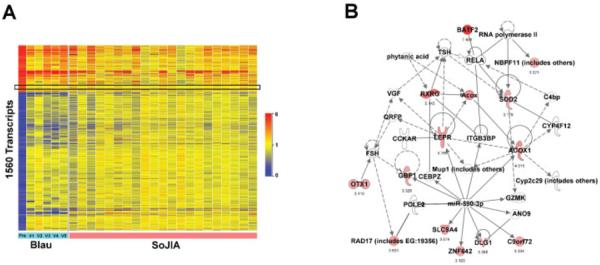
Results: Canakinumab treatment was well tolerated and led to rapid quiescence of uveitis, which had been continuously active before this treatment. Gene expression profiling analysis of the patient's blood prior to initiation of interleukin-1 (IL-1) blockade revealed differential expression of 1,993 transcripts when compared to healthy controls, and among the up-regulated transcripts, pathway analysis showed that the predominant network consisted of innate immunity-related transcripts. The transcriptional signature of the patient overlapped with the transcriptional signature of patients with systemic-onset juvenile idiopathic arthritis, and canakinumab treatment led to the normalization of most of these transcriptional changes.
Conclusion: The pathogenesis of Blau syndrome may be mediated by IL-1, and canakinumab may be useful when this disorder is unresponsive to more conventional treatments.
Copyright © 2013 by the American College of Rheumatology.
Figures


References
-
- Rose CD, Martin TM, Wouters CH. Blau syndrome revisited. Curr Opin Rheumatol. 2011;23:411–8. - PubMed
-
- Rose CD, Wouters CH, Meiorin S, Doyle TM, Davey MP, Rosenbaum JT, et al. Pediatric granulomatous arthritis: an international registry. Arthritis Rheum. 2006;54:3337–44. - PubMed
-
- Janssen CE, Rose CD, De Hertogh G, Martin TM, Bader Meunier B, Cimaz R, et al. Morphologic and immunohistochemical characterization of granulomas in the nucleotide oligomerization domain 2-related disorders Blau syndrome and Crohn disease. J Allergy Clin Immunol. 2012;129:1076–84. - PubMed
-
- Miceli-Richard C, Lesage S, Rybojad M, Prieur AM, Manouvrier-Hanu S, Hafner R, et al. CARD15 mutations in Blau syndrome. Nat Genet. 2001;29:19–20. - PubMed
-
- Fink CW, Cimaz R. Early onset sarcoidosis: not a benign disease. J Rheumatol. 1997;24:174–7. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
