

An antimicrobial stewardship program improves antimicrobial treatment by culture site and the quality of antimicrobial prescribing in critically ill patients
- PMID: 23127353
- PMCID: PMC3672592
- DOI: 10.1186/cc11854
An antimicrobial stewardship program improves antimicrobial treatment by culture site and the quality of antimicrobial prescribing in critically ill patients
Abstract
Introduction: Increasing antimicrobial costs, reduced development of novel antimicrobials, and growing antimicrobial resistance necessitate judicious use of available agents. Antimicrobial stewardship programs (ASPs) may improve antimicrobial use in intensive care units (ICUs). Our objective was to determine whether the introduction of an ASP in an ICU altered the decision to treat cultures from sterile sites compared with nonsterile sites (which may represent colonization or contamination). We also sought to determine whether ASP education improved documentation of antimicrobial use, including an explicit statement of antimicrobial regimen, indication, duration, and de-escalation.
Methods: We retrospectively analyzed consecutive patients with positive bacterial cultures admitted to a 16-bed medical-surgical ICU over 2-month periods before and after ASP introduction (April through May 2008 and 2009, respectively). We evaluated the antimicrobial treatment of positive sterile- versus nonsterile-site cultures, specified a priori. We reviewed patient charts for clinician documentation of three specific details regarding antimicrobials: an explicit statement of antimicrobial regimen/indication, duration, and de-escalation. We also analyzed cost and defined daily doses (DDDs) (a World Health Organization (WHO) standardized metric of use) before and after ASP.
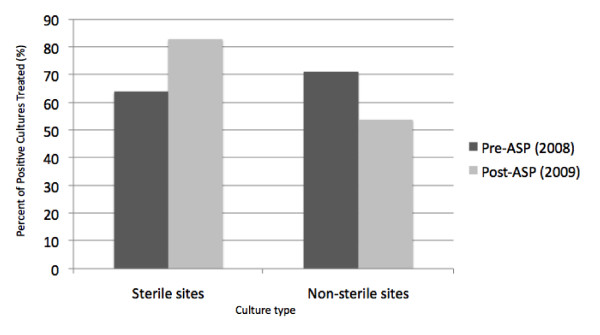
Results: Patient demographic data between the pre-ASP (n = 139) and post-ASP (n = 130) periods were similar. No difference was found in the percentage of positive cultures from sterile sites between the pre-ASP period and post-ASP period (44.9% versus 40.2%; P = 0.401). A significant increase was noted in the treatment of sterile-site cultures after ASP (64% versus 83%; P = 0.01) and a reduction in the treatment of nonsterile-site cultures (71% versus 46%; P = 0.0002). These differences were statistically significant when treatment decisions were analyzed both at an individual patient level and at an individual culture level. Increased explicit antimicrobial regimen documentation was observed after ASP (26% versus 71%; P < 0.0001). Also observed were increases in formally documented stop dates (53% versus 71%; P < 0.0001), regimen de-escalation (15% versus 23%; P = 0.026), and an overall reduction in cost and mean DDDs after ASP implementation.
Conclusions: Introduction of an ASP in the ICU was associated with improved microbiologically targeted therapy based on sterile or nonsterile cultures and improved documentation of antimicrobial use in the medical record.
Figures
References
-
- Vincent JL, Rello J, Marshall J, Silva E, Anzueto A, Martin CD, Moreno R, Lipman J, Gomersall C, Sakr Y, Reinhart K. for the EPIC-II group of investigators. International study of the prevalence and outcomes of infection in intensive care units. JAMA. 2009;16:2323–2329. doi: 10.1001/jama.2009.1754. - DOI - PubMed
-
- Gandhi TN, DePestel DD, Collins CD, Nagel J, Washer LL. Managing antimicrobial resistance in intensive care units. Crit Care Med. 2010;16:S315–S323. - PubMed
-
- Colardyn F. Appropriate and timely empirical antimicrobial treatment of ICU infections: a role for carbapenems. Acta Clin Belg. 2005;16:51–62. - PubMed
-
- Morris AM, Stewart TE, Shandling M, McIntaggart S, Liles WC. Establishing an Antimicrobial Stewardship Program. Healthcare Q. 2010;16:64–70. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
