

Primary and secondary prevention with new oral anticoagulant drugs for stroke prevention in atrial fibrillation: indirect comparison analysis
- PMID: 23129490
- PMCID: PMC3489505
- DOI: 10.1136/bmj.e7097
Primary and secondary prevention with new oral anticoagulant drugs for stroke prevention in atrial fibrillation: indirect comparison analysis
Abstract
Objective: To do an indirect comparison analysis of apixaban against dabigatran etexilate (2 doses) and rivaroxaban (1 dose), as well as of rivaroxaban against dabigatranetexilate (2 doses), for their relative efficacy and safety against each other, with particular focus on the secondary prevention population for stroke prevention in atrial fibrillation. A secondary objective was to do the same analysis in the primary prevention cohort.
Design: Indirect treatment comparisons of phase III clinical trials of stroke prevention in atrial fibrillation, with a focus on the secondary prevention cohorts. A secondary analysis was done on the primary prevention cohort.
Data sources: Medline and Central (up to June 2012), clinical trials registers, conference proceedings, and websites of regulatory agencies.
Study selection: Randomised controlled trials of rivaroxaban, dabigatran, or apixaban compared with warfarin for stroke prevention in atrial fibrillation.
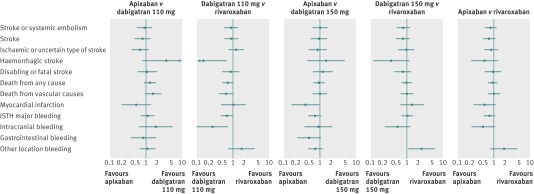
Results: In the secondary prevention (previous stroke) subgroup, when apixaban was compared with dabigatran (110 mg and 150 mg twice daily) for efficacy and safety endpoints, the only significant difference seen was less myocardial infarction (hazard ratio 0.39, 95% confidence interval 0.16 to 0.95) with apixaban compared with dabigatran 150 mg twice daily. No significant differences were seen in efficacy and most safety endpoints between apixaban or dabigatran 150 mg twice daily versus rivaroxaban. Less haemorrhagic stroke (hazard ratio 0.15, 0.03 to 0.66), vascular death (0.64, 0.42 to 0.99), major bleeding (0.68, 0.47 to 0.99), and intracranial bleeding (0.27, 0.10 to 0.73) were seen with dabigatran 110 mg twice daily versus rivaroxaban. In the primary prevention (no previous stroke) subgroup, apixaban was superior to dabigatran 110 mg twice daily for disabling or fatal stroke (hazard ratio 0.59, 0.36 to 0.97). Compared with dabigatran 150 mg twice daily, apixaban was associated with more stroke (hazard ratio 1.45, 1.01 to 2.08) and with less major bleeding (0.75, 0.60 to 0.94), gastrointestinal bleeding (0.61, 0.42 to 0.89), and other location bleeding (0.74, 0.58 to 0.94). Compared with rivaroxaban, dabigatran 110 mg twice daily was associated with more myocardial infarction events. No significant differences were seen for the main efficacy and safety endpoints between dabigatran 150 mg twice daily and rivaroxaban, or in efficacy endpoints between apixaban and rivaroxaban. Apixaban was associated with less major bleeding (hazard ratio 0.61, 0.48 to 0.78) than rivaroxaban.
Conclusions: For secondary prevention, apixaban, rivaroxaban, and dabigatran had broadly similar efficacy for the main endpoints, although the endpoints of haemorrhagic stroke, vascular death, major bleeding, and intracranial bleeding were less common with dabigatran 110 mg twice daily than with rivaroxaban. For primary prevention, the three drugs showed some differences in relation to efficacy and bleeding. These results are hypothesis generating and should be confirmed in a head to head randomised trial.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
References
-
- Potpara TS, Lip GY, Apostolakis S. New anticoagulant treatments to protect against stroke in atrial fibrillation. Heart 2012;98:1341-7. - PubMed
-
- Lip GY, Larsen TB, Skjøth F, Rasmussen LH. Indirect comparisons of new oral anticoagulant drugs for efficacy and safety when used for stroke prevention in atrial fibrillation. J Am Coll Cardiol 2012;60:738-46. - PubMed
-
- Mantha S, Ansell J. An indirect comparison of dabigatran, rivaroxaban and apixaban for atrial fibrillation. Thromb Haemost 2012;108:476-84. - PubMed
-
- Patel MR, Mahaffey KW, Garg J, Pan G, Singer DE, Hacke W, et al, for the ROCKET-AF Investigators. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med 2011;365:883-91. - PubMed
-
- Connolly SJ, Ezekowitz MD, Yusuf S, Eikelboom J, Oldgren J, Parekh A, et al, for the RE-LY Steering Committee and Investigators. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009;361:1139-51. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical