

Incremental Reduction in Risk of Death Associated With Use of Guideline-Recommended Therapies in Patients With Heart Failure: A Nested Case-Control Analysis of IMPROVE HF
- PMID: 23130115
- PMCID: PMC3487312
- DOI: 10.1161/JAHA.111.000018
Incremental Reduction in Risk of Death Associated With Use of Guideline-Recommended Therapies in Patients With Heart Failure: A Nested Case-Control Analysis of IMPROVE HF
Abstract
Background: Several therapies are guideline-recommended to reduce mortality in patients with heart failure (HF) and reduced left ventricular ejection fraction, but the incremental clinical effectiveness of these therapies has not been well studied. We aimed to evaluate the individual and incremental benefits of guideline-recommended HF therapies associated with 24-month survival.
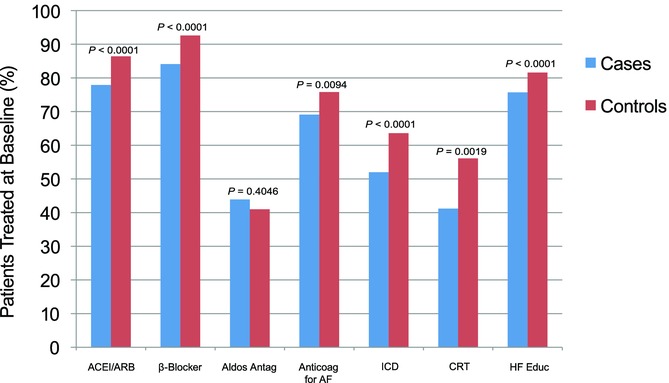
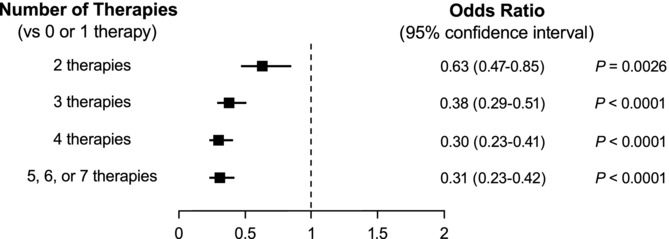
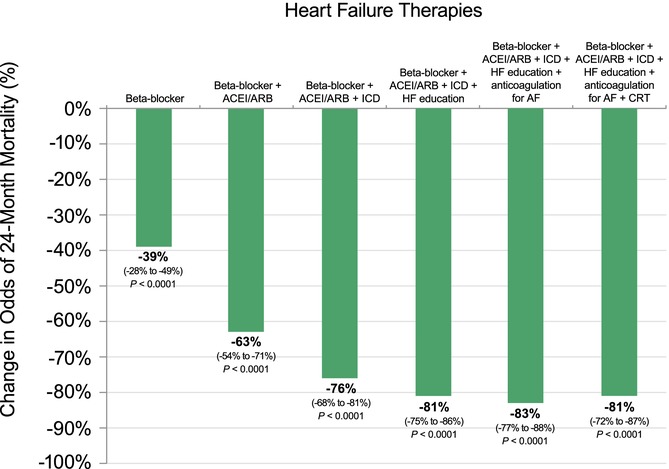
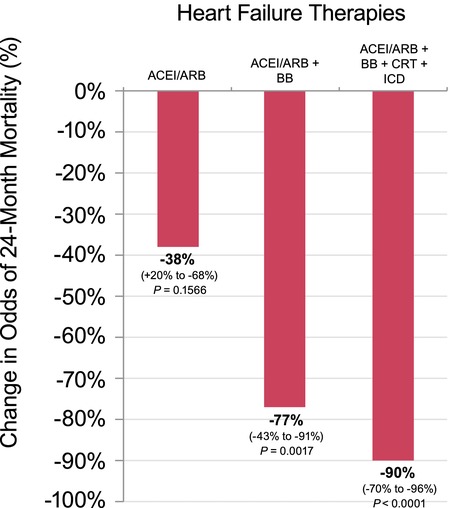
Methods and results: We performed a nested case-control study of HF patients enrolled in IMPROVE HF. Cases were patients who died within 24 months and controls were patients who survived to 24 months, propensity-matched 1:2 for multiple prognostic variables. Logistic regression was performed, and the attributable mortality risk from incomplete application of each evidence-based therapy among eligible patients was calculated. A total of 1376 cases and 2752 matched controls were identified. β-Blocker and cardiac resynchronization therapy were associated with the greatest 24-month survival benefit (adjusted odds ratio for death 0.42, 95% confidence interval (CI), 0.34-0.52; and 0.44, 95% CI, 0.29-0.67, respectively). Angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, implantable cardioverter-defibrillators, anticoagulation for atrial fibrillation, and HF education were also associated with benefit, whereas aldosterone antagonist use was not. Incremental benefits were observed with each successive therapy, plateauing once any 4 to 5 therapies were provided (adjusted odds ratio 0.31, 95% CI, 0.23-0.42 for 5 or more versus 0/1, P<0.0001).
Conclusions: Individual, with a single exception, and incremental use of guideline-recommended therapies was associated with survival benefit, with a potential plateau at 4 to 5 therapies. These data provide further rationale to implement guideline-recommended HF therapies in the absence of contraindications to patients with HF and reduced left ventricular ejection fraction. (J Am Heart Assoc. 2012;1:16-26.).
Keywords: guideline-recommended therapies; heart failure; nested case-control studies; survival benefit.
Figures
Similar articles
-
Influence of dedicated heart failure clinics on delivery of recommended therapies in outpatient cardiology practices: findings from the Registry to Improve the Use of Evidence-Based Heart Failure Therapies in the Outpatient Setting (IMPROVE HF).Am Heart J. 2010 Feb;159(2):238-44. doi: 10.1016/j.ahj.2009.11.022. Am Heart J. 2010. PMID: 20152222
-
Is heart failure guideline adherence being underestimated? The impact of therapeutic contraindications.Am Heart J. 2012 Nov;164(5):750-755.e1. doi: 10.1016/j.ahj.2012.08.002. Epub 2012 Oct 16. Am Heart J. 2012. PMID: 23137506
-
Outpatient cardiology practices with advanced practice nurses and physician assistants provide similar delivery of recommended therapies (findings from IMPROVE HF).Am J Cardiol. 2010 Jun 15;105(12):1773-9. doi: 10.1016/j.amjcard.2010.01.360. Epub 2010 May 4. Am J Cardiol. 2010. PMID: 20538129
-
How well are chronic heart failure patients being managed?Rev Cardiovasc Med. 2006;7 Suppl 1:S3-11. Rev Cardiovasc Med. 2006. PMID: 16955055 Review.
-
Strategies to improve the use of evidence-based heart failure therapies.Rev Cardiovasc Med. 2005;6 Suppl 2:S32-42. Rev Cardiovasc Med. 2005. PMID: 15891703 Review.
Cited by
-
Heart failure - what's new and what's changed?Clin Med (Lond). 2017 Jul;17(4):341-346. doi: 10.7861/clinmedicine.17-4-341. Clin Med (Lond). 2017. PMID: 28765411 Free PMC article. Review.
-
New pharmacological treatments for heart failure with reduced ejection fraction (HFrEF): A Bayesian network meta-analysis.Medicine (Baltimore). 2020 Jan;99(5):e18341. doi: 10.1097/MD.0000000000018341. Medicine (Baltimore). 2020. PMID: 32000355 Free PMC article.
-
Managing patients with heart failure: contemporary real-world experience.BMC Res Notes. 2022 Feb 10;15(1):41. doi: 10.1186/s13104-022-05938-z. BMC Res Notes. 2022. PMID: 35144677 Free PMC article.
-
Analysis of Outcomes in Ischemic vs Nonischemic Cardiomyopathy in Patients With Atrial Fibrillation: A Report From the GARFIELD-AF Registry.JAMA Cardiol. 2019 Jun 1;4(6):526-548. doi: 10.1001/jamacardio.2018.4729. JAMA Cardiol. 2019. PMID: 31066873 Free PMC article.
-
Trends in heart failure hospitalizations.Curr Heart Fail Rep. 2012 Dec;9(4):346-53. doi: 10.1007/s11897-012-0117-5. Curr Heart Fail Rep. 2012. PMID: 23070579 Review.
References
-
- Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG, Jessup M, Konstam MA, Mancini DM, Michl K, Oates JA, Rahko PS, Silver MA, Stevenson LW, Yancy CW, Antman EM, Smith SC, Jr, Adams CD, Anderson JL, Faxon DP, Fuster V, Halperin JL, Hiratzka LF, Jacobs AK, Nishimura R, Ornato JP, Page RL, Riegel B. ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to update the 2001 Guidelines for the Evaluation and Management of Heart Failure): developed in collaboration with the American College of Chest Physicians and the International Society for Heart and Lung Transplantation: endorsed by the Heart Rhythm Society. Circulation. 2005;112:e154–e235. - PubMed
-
- Jessup M, Abraham WT, Casey DE, Feldman AM, Francis GS, Ganiats TG, Konstam MA, Mancini DM, Rahko PS, Silver MA, Stevenson LW, Yancy CW. 2009 focused update: ACCF/AHA guidelines for the diagnosis and management of heart failure in adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation. 2009;119:1977–2016. - PubMed
-
- Heart Failure Society of America. Lindenfeld J, Albert NM, Boehmer JP, Collins SP, Ezekowitz JA, Givertz MM, Katz SD, Klapholz M, Moser DK, Rogers JG, Starling RC, Stevenson WG, Tang WH, Teerlink JR, Walsh MN. HFSA 2010 comprehensive heart failure practice guideline. J Card Fail. 2010;16:e1–e194. - PubMed
-
- Task Force for Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of European Society of Cardiology. Dickstein K, Cohen-Solal A, Filippatos G, McMurray JJ, Ponikowski P, Poole-Wilson PA, Strömberg A, van Veldhuisen DJ, Atar D, Hoes AW, Keren A, Mebazaa A, Nieminen M, Priori SG, Swedberg K, ESC Committee for Practice Guidelines. Vahanian A, Camm J, De Caterina R, Dean V, Dickstein K, Filippatos G, Funck-Brentano C, Hellemans I, Kristensen SD, McGregor K, Sechtem U, Silber S, Tendera M, Widimsky P, Zamorano JL. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM) Eur Heart J. 2008;29:2388–2442. - PubMed
-
- Committee on Comparative Effectiveness Research Prioritization, Institute of Medicine. Initial National Priorities for Comparative Effectiveness Research. Washington, DC: National Academies Press; 2009. http://www.nap.edu/catalog.php?record_id=12648. Accessed August 24, 2011.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
