

Relationship of national institutes of health stroke scale to 30-day mortality in medicare beneficiaries with acute ischemic stroke
- PMID: 23130117
- PMCID: PMC3487316
- DOI: 10.1161/JAHA.111.000034
Relationship of national institutes of health stroke scale to 30-day mortality in medicare beneficiaries with acute ischemic stroke
Abstract
Background: The National Institutes of Health Stroke Scale (NIHSS), a well-validated tool for assessing initial stroke severity, has previously been shown to be associated with mortality in acute ischemic stroke. However, the relationship, optimal categorization, and risk discrimination with the NIHSS for predicting 30-day mortality among Medicare beneficiaries with acute ischemic stroke has not been well studied.
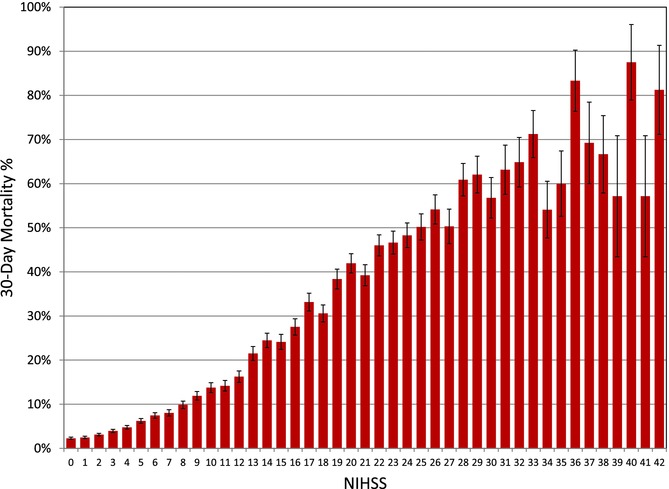
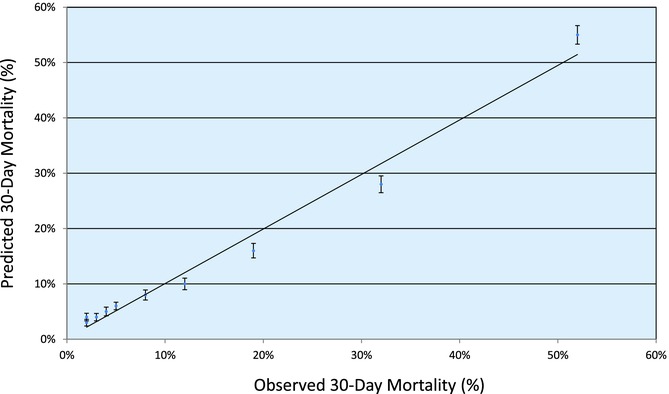
Methods and results: We analyzed data from 33102 fee-for-service Medicare beneficiaries treated at 404 Get With The Guidelines-Stroke hospitals between April 2003 and December 2006 with NIHSS documented. The 30-day mortality rate by NIHSS as a continuous variable and by risk-tree determined or prespecified categories were analyzed, with discrimination of risk quantified by the c-statistic. In this cohort, mean age was 79.0 years and 58% were female. The median NIHSS score was 5 (25th to 75th percentile 2 to 12). There were 4496 deaths in the first 30 days (13.6%). There was a strong graded relation between increasing NIHSS score and higher 30-day mortality. The 30-day mortality rates for acute ischemic stroke by NIHSS categories were as follows: 0 to 7, 4.2%; 8 to 13, 13.9%; 14 to 21, 31.6%; 22 to 42, 53.5%. A model with NIHSS alone provided excellent discrimination whether included as a continuous variable (c-statistic 0.82 [0.81 to 0.83]), 4 categories (c-statistic 0.80 [0.79 to 0.80]), or 3 categories (c-statistic 0.79 [0.78 to 0.79]).
Conclusions: The NIHSS provides substantial prognostic information regarding 30-day mortality risk in Medicare beneficiaries with acute ischemic stroke. This index of stroke severity is a very strong discriminator of mortality risk, even in the absence of other clinical information, whether used as a continuous or categorical risk determinant. (J Am Heart Assoc. 2012;1:42-50.).
Keywords: National Institutes of Health Stroke Scale; ischemic stroke; mortality; registries.
Figures

References
-
- Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, Moy CS, Mozaffarian D, Mussolino ME, Nichol G, Paynter NP, Soliman EZ, Sorlie PD, Sotoodehnia N, Turan TN, Virani SS, Wong ND, Woo D, Turner MB. on behalf of the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics 2012 update: a report from the American Heart Association. Circulation. 2012;125:e2–e220. - PMC - PubMed
-
- Krumholz HM, Normand SL, Spertus JA, Shahian DM, Bradley EH. Measuring performance for treating heart attacks and heart failure: the case for outcomes measurement. Health Aff (Millwood) 2007;26:75–85. - PubMed
-
- Krumholz HM, Normand SL. Public reporting of 30-day mortality for patients hospitalized with acute myocardial infarction and heart failure. Circulation. 2008;118:1394–1397. - PubMed
-
- Lindenauer PK, Bernheim SM, Grady JN, Lin Z, Wang Y, Wang Y, Merrill AR, Han LF, Rapp MT, Drye EE, Normand SL, Krumholz HM. The performance of US hospitals as reflected in risk-standardized 30-day mortality and readmission rates for medicare beneficiaries with pneumonia. J Hosp Med. 2010;5:E12–18. - PubMed
-
- Hospital Compare. 2011. Department of Health and Human Services. http://www.hospitalcompare.hhs.gov. Accessed August 24.
LinkOut - more resources
Full Text Sources
Miscellaneous
