

Carotid Intima-Media Thickness Progression in HIV-Infected Adults Occurs Preferentially at the Carotid Bifurcation and Is Predicted by Inflammation
- PMID: 23130122
- PMCID: PMC3487373
- DOI: 10.1161/JAHA.111.000422
Carotid Intima-Media Thickness Progression in HIV-Infected Adults Occurs Preferentially at the Carotid Bifurcation and Is Predicted by Inflammation
Abstract
Background: Shear stress gradients and inflammation have been causally associated with atherosclerosis development in carotid bifurcation regions. The mechanism underlying higher levels of carotid intima-media thickness observed among HIV-infected individuals remains unknown.
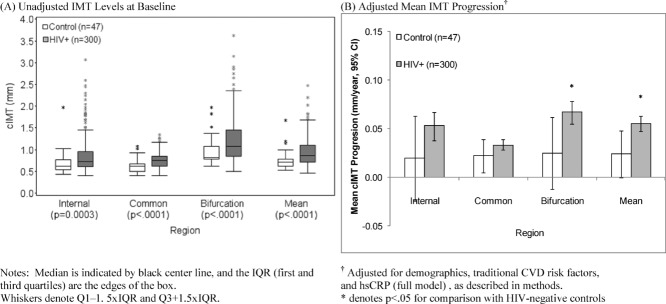
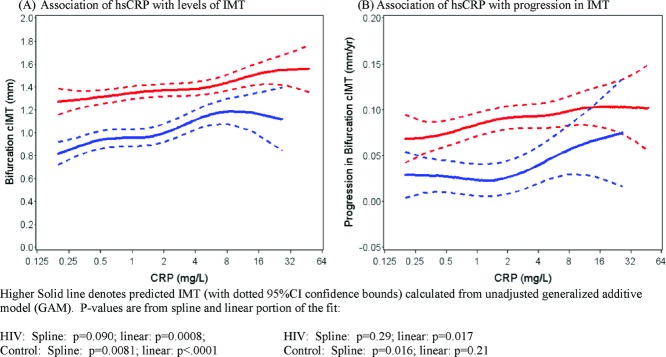
Methods and results: We measured carotid intima-media thickness progression and development of plaque in the common carotid, bifurcation region, and internal carotid artery in 300 HIV-infected persons and 47 controls. The median duration of follow-up was 2.4 years. When all segments were included, the rate of intima-media thickness progression was greater in HIV-infected subjects compared with controls after adjustment for traditional risk factors (0.055 vs. 0.024 mm/year, P=0.016). Rate of progression was also greater in the bifurcation region (0.067 vs. 0.025 mm/year, P=0.042) whereas differences were smaller in the common and internal regions. HIV-infected individuals had a greater incidence of plaque compared with controls in the internal (23% vs. 6.4%, P=0.0037) and bifurcation regions (34% vs. 17%, P=0.014). Among HIV-infected individuals, the rate of progression in the bifurcation region was more rapid compared with the common carotid, internal, or mean intima-media thickness; in contrast, progression rates among controls were similar at all sites. Baseline hsCRP was elevated in HIV-infected persons and was a predictor of progression in the bifurcation region.
Conclusions: Atherosclerosis progresses preferentially in the carotid bifurcation region in HIV-infected individuals. hsCRP, a marker of inflammation, is elevated in HIV and is associated with progression in the bifurcation region. These data are consistent with a model in which the interplay between hemodynamic shear stresses and HIV-associated inflammation contribute to accelerated atherosclerosis. (J Am Heart Assoc. 2012;1:jah3-e000422 doi: 10.1161/JAHA.111.000422.)
Clinical trial registration: URL: http://clinicaltrials.gov. Unique identifier: NCT01519141.
Keywords: AIDS; atherosclerosis; carotid arteries; inflammation.
Figures
Comment in
-
HIV and Cardiovascular Disease: We Need a Mechanism, and We Need a Plan.J Am Heart Assoc. 2016 Mar 24;4(3):e003411. doi: 10.1161/JAHA.116.003411. J Am Heart Assoc. 2016. PMID: 27013540 Free PMC article. No abstract available.
References
-
- Klein D, Hurley LB, Quesenberry CP, Jr, Sidney S. Do protease inhibitors increase the risk for coronary heart disease in patients with HIV-1 infection?. J Acquir Immune Defic Syndr. 2002;30:471-477 - PubMed
-
- Hsue PY, Giri K, Erickson S, MacGregor JS, Younes N, Shergill A, Waters DD. Clinical features of acute coronary syndromes in patients with human immunodeficiency virus infection. Circulation. 2004;109:316-319 - PubMed
-
- Lorenz MW, Stephan C, Harmjanz A, Staszewski S, Buehler A, Bickel M, Kegler S, Ruhkamp D, Steinmetz H, Sitzer M. Both long-term HIV infection and highly active antiretroviral therapy are independent risk factors for early carotid atherosclerosis. Atherosclerosis. 2008;196:720-726 - PubMed
-
- Hsue PY, Lo JC, Franklin A, Bolger AF, Martin JN, Deeks SG, Waters DD. Progression of atherosclerosis as assessed by carotid intima-media thickness in patients with HIV infection. Circulation. 2004;109:1603-1608 - PubMed
