

Vulnerable myocardial interstitium in patients with isolated left ventricular hypertrophy and sudden cardiac death: a postmortem histological evaluation
- PMID: 23130141
- PMCID: PMC3487319
- DOI: 10.1161/JAHA.112.001511
Vulnerable myocardial interstitium in patients with isolated left ventricular hypertrophy and sudden cardiac death: a postmortem histological evaluation
Abstract
Background: Concentric left ventricular hypertrophy (LVH) is independently associated with increased risk of sudden cardiac death (SCD). Some animal models of LVH display specific alterations of the myocardial interstitium that could increase myocardial vulnerability to ventricular arrhythmias, but these merit evaluation in humans with LVH and SCD.
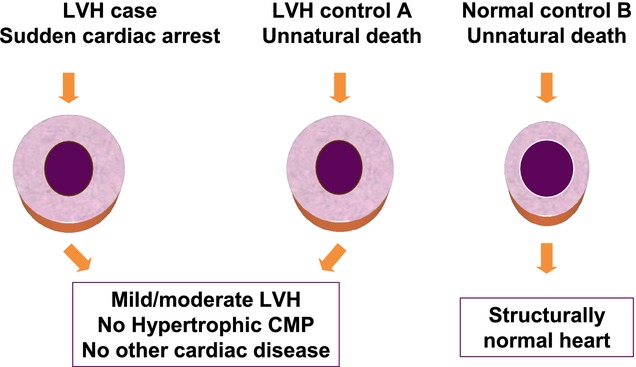
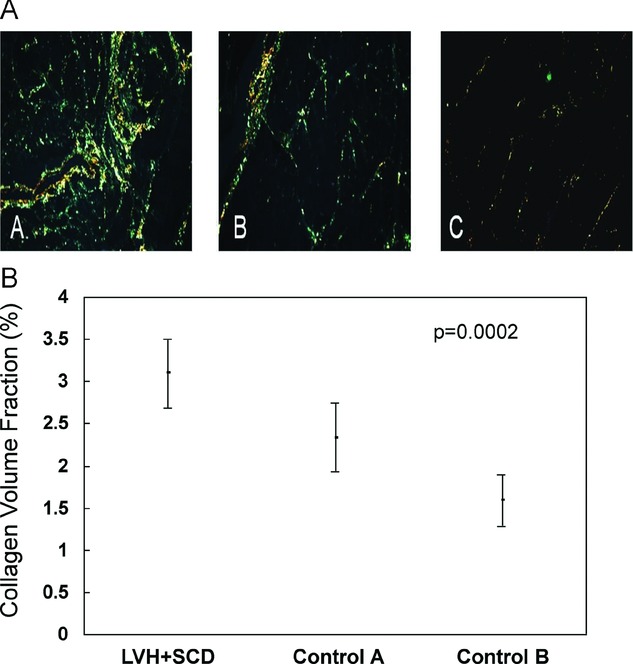
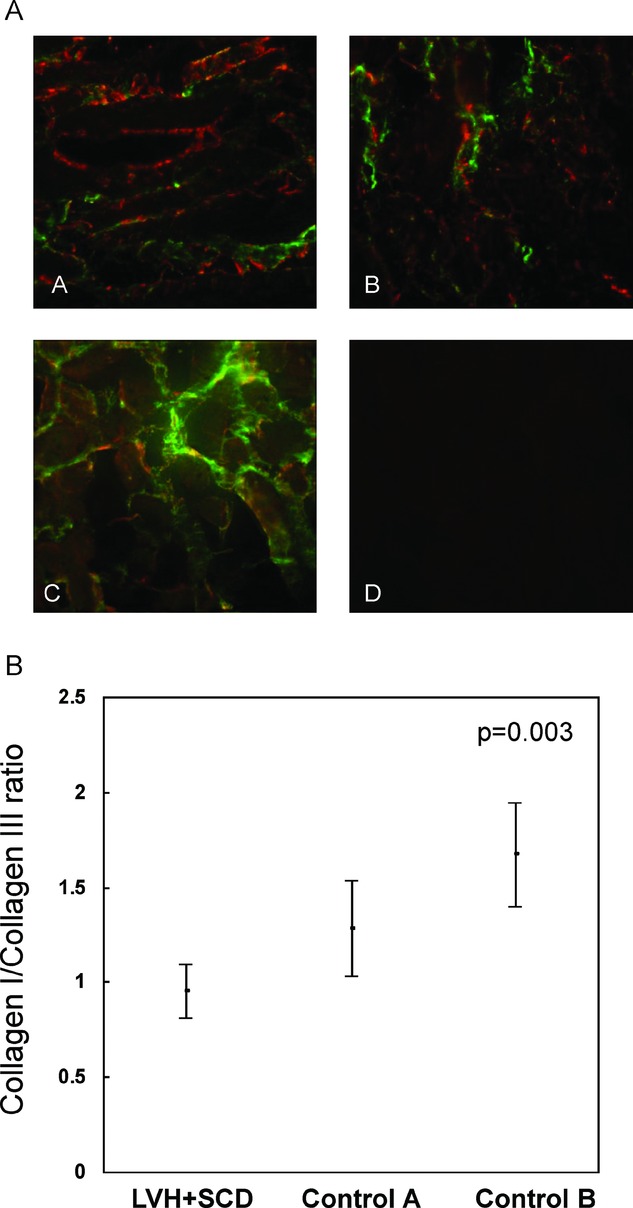
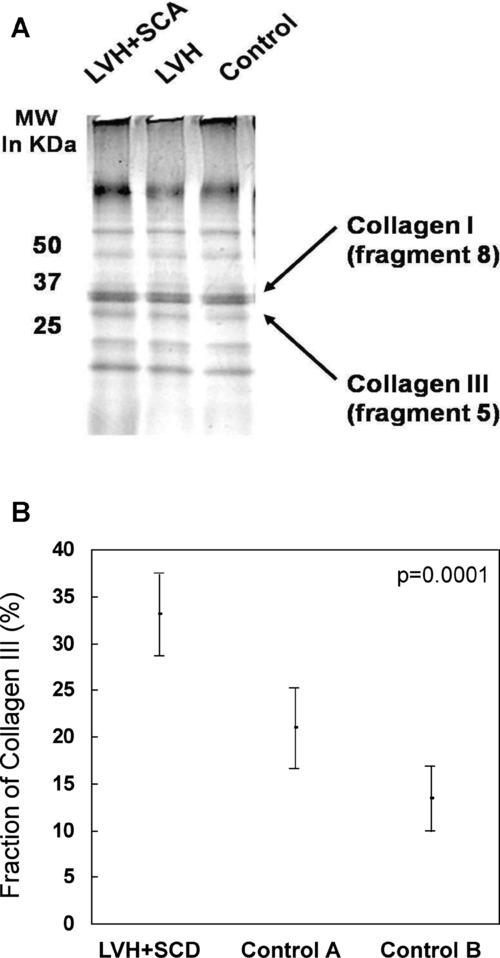
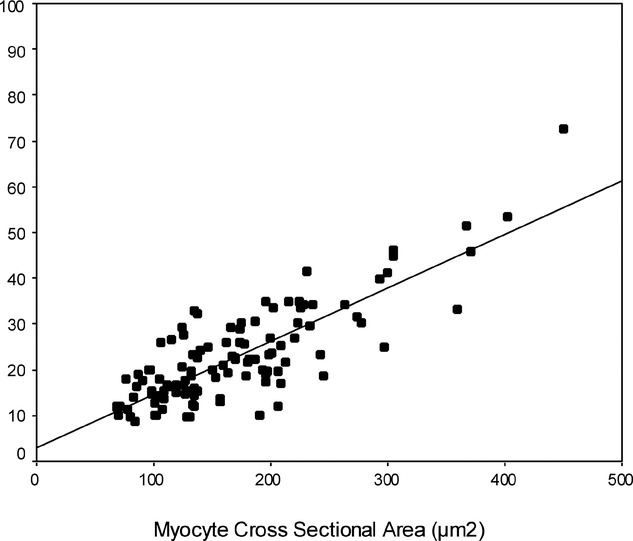
Methods and results: Twelve consecutive patients with isolated LVH and SCD (LVH+SCD) in the absence of hypertrophic cardiomyopathy, coronary disease, or other cardiac structural abnormality were ascertained in the Oregon Sudden Unexpected Death Study. Detailed postmortem comparisons were conducted with 18 controls who had isolated LVH and unnatural deaths (Control Group A) and 6 controls who had structurally normal hearts and unnatural deaths (Control Group B). Postmortem left ventricular myocardial sections were obtained for measurement of collagen volume fraction, characterization of gap junctions, and quantification of collagen subtypes. Heart weight normalized to body weight was higher in LVH+SCD cases (6.9±1.2 g/kg) than in Control Group A (5.3±1.4 g/kg) and Control Group B (4.2±0.3 g/kg); P=0.001. Collagen volume fraction was also higher in LVH+SCD cases (3.1±0.4) than in Control Group A (2.3±0.4) and Control Group B (1.6±0.3); P=0.0002. The relative amount of collagen III was significantly higher in LVH+SCD cases (33.0±4.4%) than in Control Group A (20.9±4.3%) and Control Group B (13.4±3.5%); P=0.0001. There was an overall increase in the number of connexin 43-labeled gap junctions with increasing myocyte size. No subject was found to have high-risk hypertrophic cardiomyopathy mutations.
Conclusions: In addition to the expected increase in myocardial mass and overall collagen content, SCD with isolated LVH was associated with relative abundance of type III collagen, a novel finding that warrants further mechanistic evaluation. (J Am Heart Assoc. 2012;1:e001511 doi: 10.1161/JAHA.111.001511.).
Keywords: collagen; death, sudden; hypertrophy; myocardium; remodeling.
Figures
References
-
- Haider AW, Larson MG, Benjamin EJ, Levy D. Increased left ventricular mass and hypertrophy are associated with increased risk for sudden death. J Am Coll Cardiol. 1998;32:1454-1459 - PubMed
-
- Levy D, Anderson KM, Savage DD, Balkus SA, Kannel WB, Castelli WP. Risk of ventricular arrhythmias in left ventricular hypertrophy: the Framingham Heart Study. Am J Cardiol. 1987;60:560-565 - PubMed
-
- Fishman GI, Chugh SS, Dimarco JP, Albert CM, Anderson ME, Bonow RO, Buxton AE, Chen PS, Estes M, Jouven X, Kwong R, Lathrop DA, Mascette AM, Nerbonne JM, O'Rourke B, Page RL, Roden DM, Rosenbaum DS, Sotoodehnia N, Trayanova NA, Zheng ZJ. Sudden cardiac death prediction and prevention: report from a National Heart, Lung, and Blood Institute and Heart Rhythm Society Workshop. Circulation. 2010;122:2335-2348 - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
