

Reduction of ischemia/reperfusion injury with bendavia, a mitochondria-targeting cytoprotective Peptide
- PMID: 23130143
- PMCID: PMC3487333
- DOI: 10.1161/JAHA.112.001644
Reduction of ischemia/reperfusion injury with bendavia, a mitochondria-targeting cytoprotective Peptide
Abstract
Background: Manifestations of reperfusion injury include myocyte death leading to infarction, contractile dysfunction, and vascular injury characterized by the "no-reflow" phenomenon. Mitochondria-produced reactive oxygen species are believed to be centrally involved in each of these aspects of reperfusion injury, although currently no therapies reduce reperfusion injury by targeting mitochondria specifically.
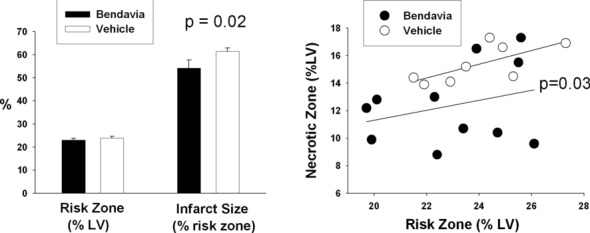
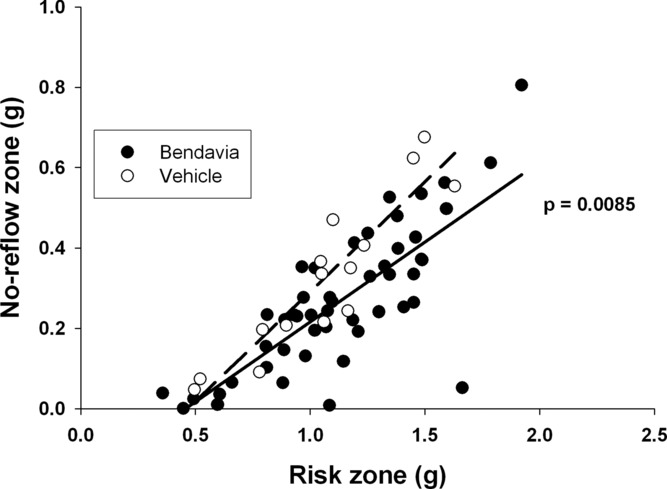
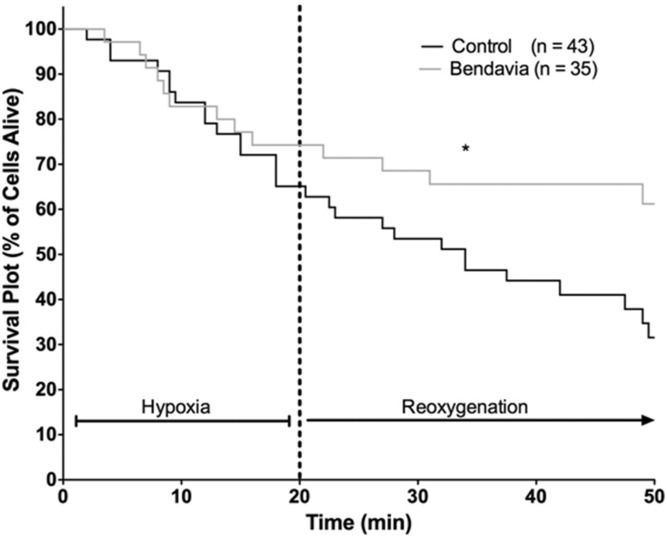
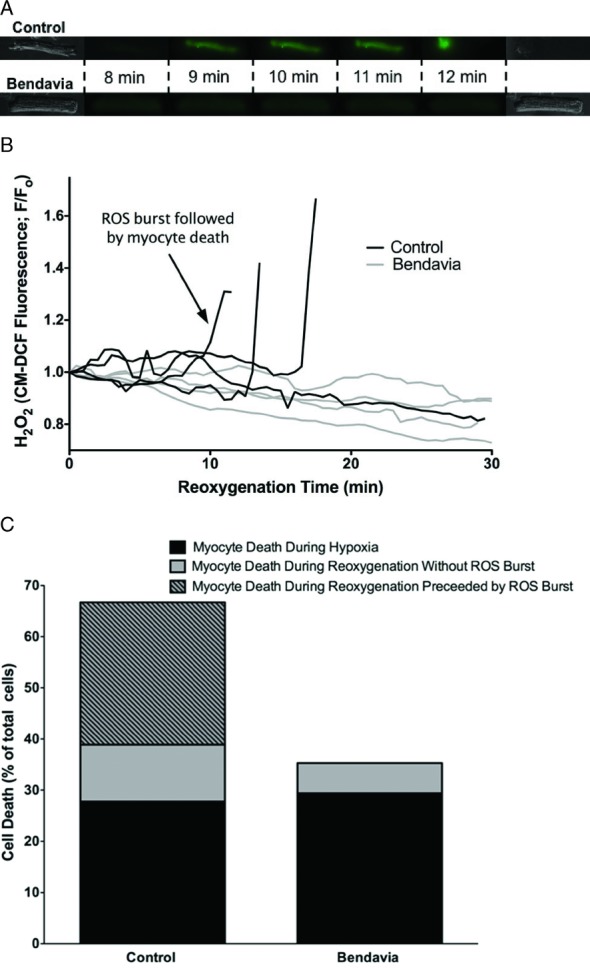
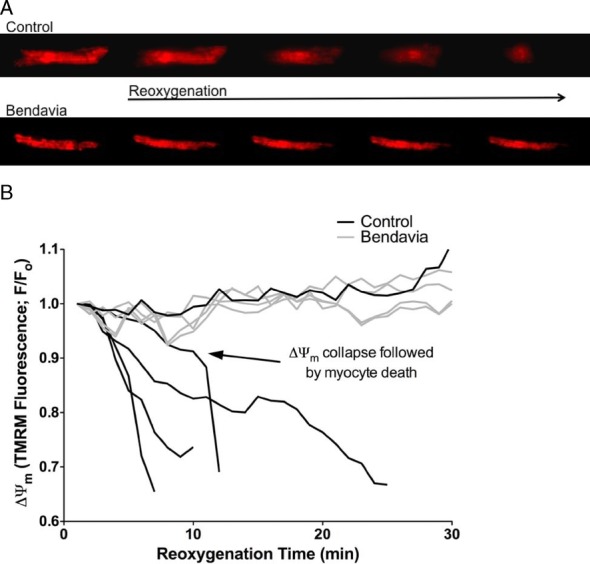
Methods and results: We investigated the cardioprotective effects of a mitochondria-targeted peptide, Bendavia (Stealth Peptides), across a spectrum of experimental cardiac ischemia/reperfusion models. Postischemic administration of Bendavia reduced infarct size in an in vivo sheep model by 15% (P=0.02) and in an ex vivo guinea pig model by 38% to 42% (P<0.05). In an in vivo rabbit model, the extent of coronary no-reflow was assessed with Thioflavin S staining and was significantly smaller in the Bendavia group for any given ischemic risk area than in the control group (P=0.0085). Myocardial uptake of Bendavia was ≈25% per minute, and uptake remained consistent throughout reperfusion. Postischemic recovery of cardiac hemodynamics was not influenced by Bendavia in any of the models studied. Isolated myocytes exposed to hypoxia/reoxygenation showed improved survival when treated with Bendavia. This protection appeared to be mediated by lowered reactive oxygen species-mediated cell death during reoxygenation, associated with sustainment of mitochondrial membrane potential in Bendavia-treated myocytes.
Conclusions: Postischemic administration of Bendavia protected against reperfusion injury in several distinct models of injury. These data suggest that Bendavia is a mitochondria-targeted therapy that reduces reperfusion injury by maintaining mitochondrial energetics and suppressing cellular reactive oxygen species levels. (J Am Heart Assoc. 2012;1:e001644 doi: 10.1161/JAHA.112.001644.).
Keywords: cardioprotection; infarction; mitochondria; peptide.
Figures



Similar articles
-
Reduction of early reperfusion injury with the mitochondria-targeting peptide bendavia.J Cardiovasc Pharmacol Ther. 2014 Jan;19(1):121-32. doi: 10.1177/1074248413508003. Epub 2013 Nov 28. J Cardiovasc Pharmacol Ther. 2014. PMID: 24288396 Free PMC article.
-
The Mitochondria-targeted Peptide, Bendavia, Attenuated Ischemia/Reperfusion-induced Stroke Damage.Neuroscience. 2020 Sep 1;443:110-119. doi: 10.1016/j.neuroscience.2020.07.044. Epub 2020 Jul 30. Neuroscience. 2020. PMID: 32738431
-
Cardioprotective effects of idebenone do not involve ROS scavenging: Evidence for mitochondrial complex I bypass in ischemia/reperfusion injury.J Mol Cell Cardiol. 2019 Oct;135:160-171. doi: 10.1016/j.yjmcc.2019.08.010. Epub 2019 Aug 22. J Mol Cell Cardiol. 2019. PMID: 31445917
-
The reduction of infarct size--forty years of research.Rev Port Cardiol. 2010 Jun;29(6):1037-53. Rev Port Cardiol. 2010. PMID: 20964114 Review. English, Portuguese.
-
Is further improvement of the treatment of acute coronary syndromes still possible?Postepy Kardiol Interwencyjnej. 2013;9(1):41-4. doi: 10.5114/pwki.2013.34027. Epub 2013 Mar 21. Postepy Kardiol Interwencyjnej. 2013. PMID: 24570690 Free PMC article. Review.
Cited by
-
The cardiolipin-binding peptide elamipretide mitigates fragmentation of cristae networks following cardiac ischemia reperfusion in rats.Commun Biol. 2020 Jul 17;3(1):389. doi: 10.1038/s42003-020-1101-3. Commun Biol. 2020. PMID: 32680996 Free PMC article.
-
Perspectives on mitochondrial relevance in cardiac ischemia/reperfusion injury.Front Cell Dev Biol. 2022 Dec 6;10:1082095. doi: 10.3389/fcell.2022.1082095. eCollection 2022. Front Cell Dev Biol. 2022. PMID: 36561366 Free PMC article. Review.
-
Combined Therapy with SS31 and Mitochondria Mitigates Myocardial Ischemia-Reperfusion Injury in Rats.Int J Mol Sci. 2018 Sep 15;19(9):2782. doi: 10.3390/ijms19092782. Int J Mol Sci. 2018. PMID: 30223594 Free PMC article.
-
Translational issues for mitoprotective agents as adjunct to reperfusion therapy in patients with ST-segment elevation myocardial infarction.J Cell Mol Med. 2020 Mar;24(5):2717-2729. doi: 10.1111/jcmm.14953. Epub 2020 Jan 22. J Cell Mol Med. 2020. PMID: 31967733 Free PMC article. Review.
-
Phase 2a Clinical Trial of Mitochondrial Protection (Elamipretide) During Stent Revascularization in Patients With Atherosclerotic Renal Artery Stenosis.Circ Cardiovasc Interv. 2017 Sep;10(9):e005487. doi: 10.1161/CIRCINTERVENTIONS.117.005487. Circ Cardiovasc Interv. 2017. PMID: 28916603 Free PMC article. Clinical Trial.
References
-
- Herlitz J, Bengtson A, Hjalmarson A, Karlson BW. Morbidity during five years after myocardial infarction and its relation to infarct size. Clin Cardiol. 1988;11:672-677 - PubMed
-
- Herlitz J, Hjalmarson A, Waldenstrom J. Relationship between enzymatically estimated infarct size and short- and long-term survival after acute myocardial infarction. Acta Med Scand. 1984;216:261-267 - PubMed
-
- Miller TD, Christian TF, Hopfenspirger MR, Hodge DO, Gersh BJ, Gibbons RJ. Infarct size after acute myocardial infarction measured by quantitative tomographic 99mTc sestamibi imaging predicts subsequent mortality. Circulation. 1995;92:334-341 - PubMed
-
- Ndrepepa G, Tiroch K, Fusaro M, Keta D, Seyfarth M, Byrne RA, Pache J, Alger P, Mehilli J, Schomig A, Kastrati A. 5-year prognostic value of no-reflow phenomenon after percutaneous coronary intervention in patients with acute myocardial infarction. J Am Coll Cardiol. 2010;55:2383-2389 - PubMed
-
- Rezkalla SH, Dharmashankar KC, Abdalrahman IB, Kloner RA. No-reflow phenomenon following percutaneous coronary intervention for acute myocardial infarction: incidence, outcome, and effect of pharmacologic therapy. J Interv Cardiol. 2010;23:429-436 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
