

Patterns, predictors, variations, and temporal trends in emergency medical service hospital prenotification for acute ischemic stroke
- PMID: 23130167
- PMCID: PMC3487363
- DOI: 10.1161/JAHA.112.002345
Patterns, predictors, variations, and temporal trends in emergency medical service hospital prenotification for acute ischemic stroke
Abstract
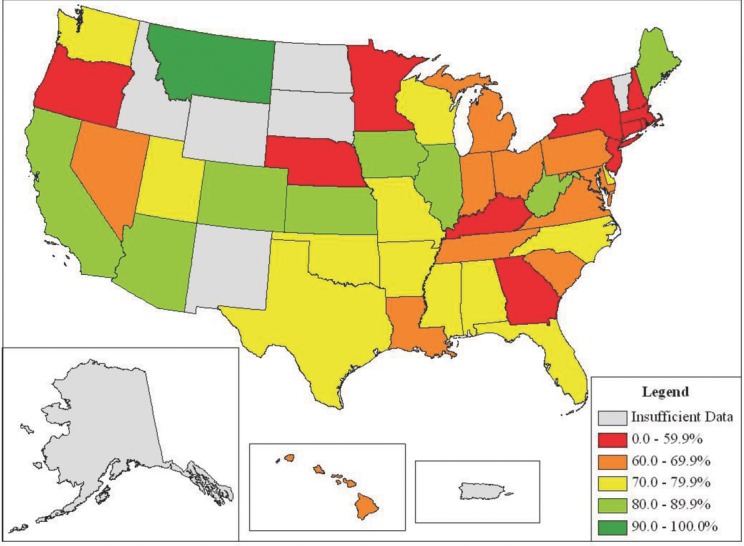
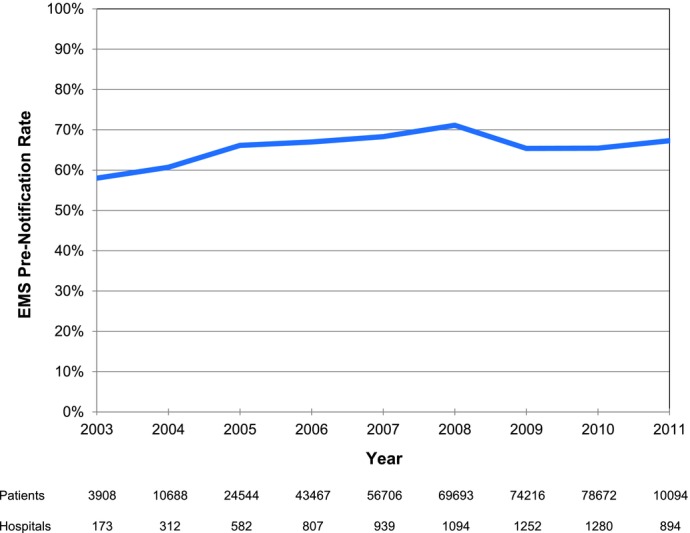
BACKGROUND#ENTITYSTARTX02014;: Emergency medical services (EMS) hospital prenotification of an incoming stroke patient is guideline recommended as a means of increasing the timeliness with which stroke patients are evaluated and treated. Still, data are limited with regard to national use of, variations in, and temporal trends in EMS prenotification and associated predictors of its use. METHODS AND RESULTS#ENTITYSTARTX02014;: We examined 371 988 patients with acute ischemic stroke who were transported by EMS and enrolled in 1585 hospitals participating in Get With The Guidelines-Stroke from April 1, 2003, through March 31, 2011. Prenotification occurred in 249 197 EMS-transported patients (67.0%) and varied widely by hospital (range, 0% to 100%). Substantial variations by geographic regions and by state, ranging from 19.7% in Washington, DC, to 93.4% in Montana, also were noted. Patient factors associated with lower use of prenotification included older age, diabetes mellitus, and peripheral vascular disease. Prenotification was less likely for black patients than for white patients (adjusted odds ratio 0.94, 95% confidence interval 0.92-0.97, P<0.0001). Hospital factors associated with greater EMS prenotification use were absence of academic affiliation, higher annual volume of tissue plasminogen activator administration, and geographic location outside the Northeast. Temporal improvements in prenotification rates showed a modest general increase, from 58.0% in 2003 to 67.3% in 2011 (P temporal trend <0.0001). CONCLUSIONS#ENTITYSTARTX02014;: EMS hospital prenotification is guideline recommended, yet among patients transported to Get With The Guidelines-Stroke hospitals it is not provided for 1 in 3 EMS-arriving patients with acute ischemic stroke and varies substantially by hospital, state, and region. These results support the need for enhanced implementation of stroke systems of care. (J Am Heart Assoc. 2012;1:e002345 doi: 10.1161/JAHA.112.002345.).
Keywords: emergency medicine; hospitals; registries; stroke.
Figures
References
-
- Towfighi A, Saver JL. Stroke declines from third to fourth leading cause of death in the United States: historical perspective and challenges ahead. Stroke. 2011;42:2351-2355 - PubMed
-
- Adams HP, Jr, del Zoppo G, Alberts MJ, Bhatt DL, Brass L, Furlan A, Grubb RL, Higashida RT, Jauch EC, Kidwell C, Lyden PD, Morgenstern LB, Qureshi AI, Rosenwasser RH, Scott PA, Wijdicks EF. Guidelines for the early management of adults with ischemic stroke. Circulation. 2007;115:e478-e534 - PubMed
-
- National Institute of Neurological Disorders and Stroke rt‐PA Stroke Study Group Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. 1995;333:1581-1587 - PubMed
-
- Lees KR, Bluhmki E, von Kummer R, Brott TG, Toni D, Grotta JC, Albers GW, Kaste M, Marler JR, Hamilton SA, Tilley BC, Davis SM, Donnan GA, Hacke W, ECASS, ATLANTIS, NINDS and EPITHET rt‐PA Study Group. Allen K, Mau J, Meier D, del Zoppo G, De Silva DA, Butcher KS, Parsons MW, Barber PA, Levi C, Bladin C, Byrnes G. Time to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet. 2010;375:1695-1703 - PubMed
-
- Fonarow GC, Smith EE, Saver JL, Reeves MJ, Bhatt DL, Grau‐Sepulveda MV, Olson DM, Hernandez AF, Peterson ED, Schwamm LH. Timeliness of tissue‐type plasminogen activator therapy in acute ischemic stroke: patient characteristics, hospital factors, and outcomes associated with door‐to‐needle times within 60 minutes. Circulation. 2011;123:750-758 - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
