

Emerging concepts in the diagnosis and treatment of patients with undifferentiated angioedema
- PMID: 23131076
- PMCID: PMC3518251
- DOI: 10.1186/1865-1380-5-39
Emerging concepts in the diagnosis and treatment of patients with undifferentiated angioedema
Abstract
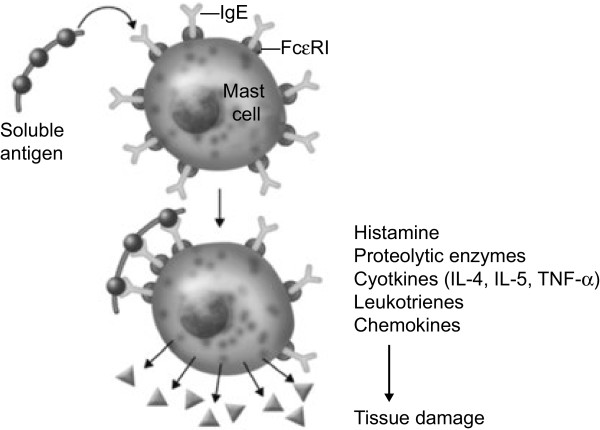
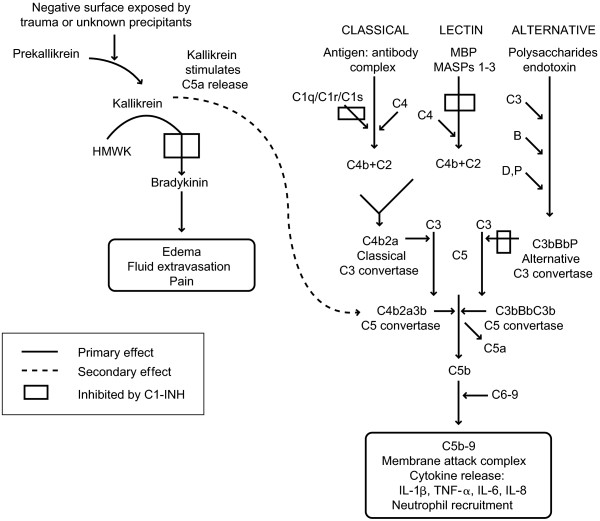
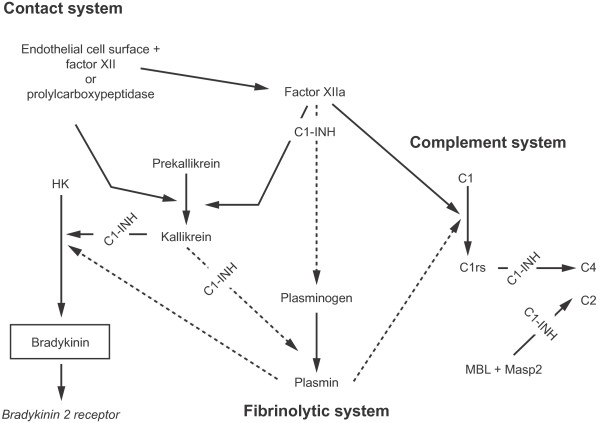
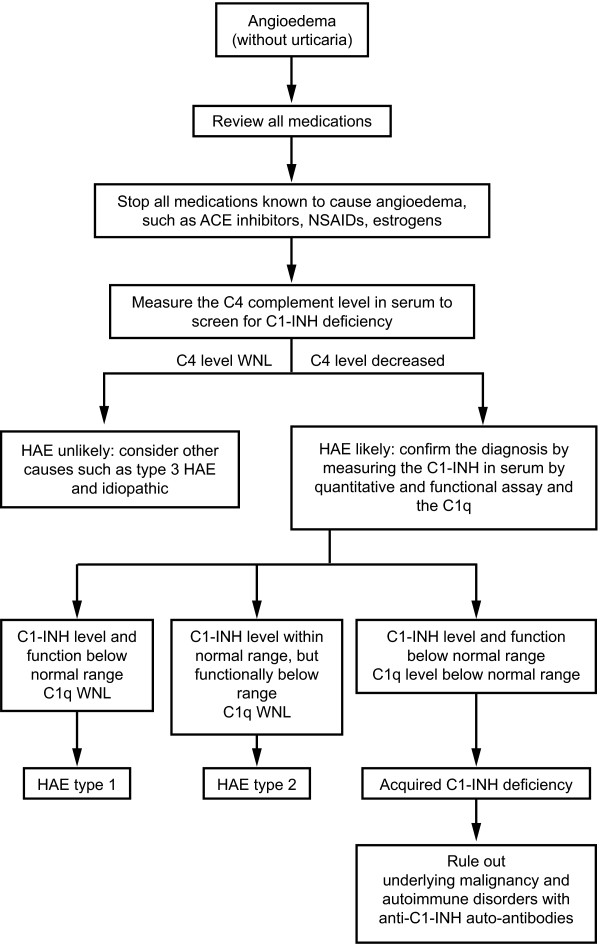
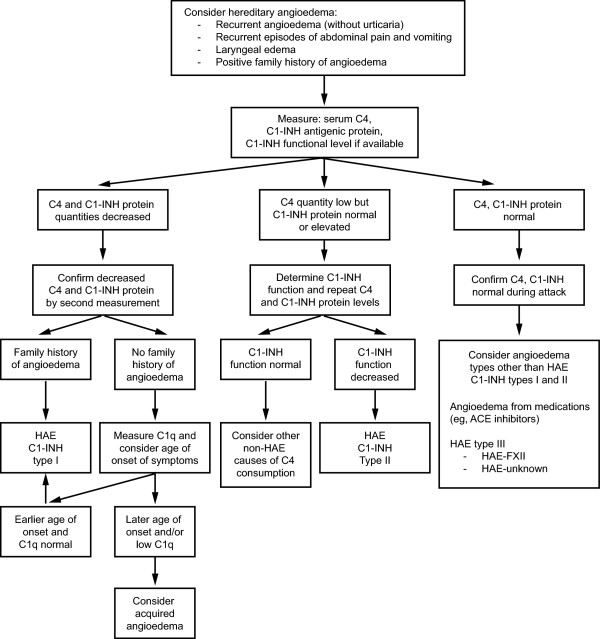
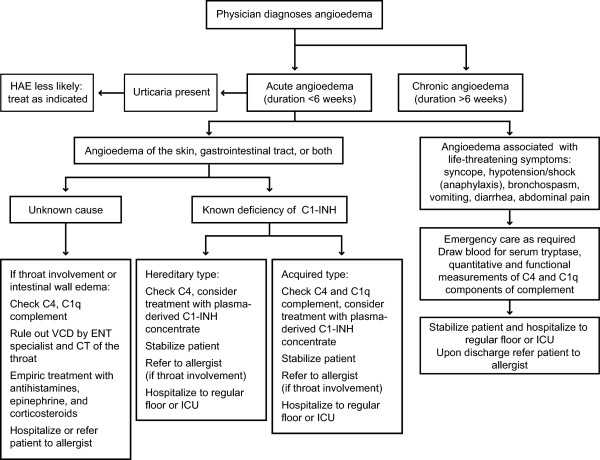
Angioedema is a sudden, transient swelling of well-demarcated areas of the dermis, subcutaneous tissue, mucosa, and submucosal tissues that can occur with or without urticaria. Up to 25% of people in the US will experience an episode of urticaria or angioedema during their lifetime, and many will present to the emergency department with an acute attack. Most cases of angioedema are attributable to the vasoactive mediators histamine and bradykinin. Histamine-mediated (allergic) angioedema occurs through a type I hypersensitivity reaction, whereas bradykinin-mediated (non-allergic) angioedema is iatrogenic or hereditary in origin.Although their clinical presentations bear similarities, the treatment algorithm for histamine-mediated angioedema differs significantly from that for bradykinin-mediated angioedema. Corticosteroids, and epinephrine are effective in the management of histamine-mediated angioedema but are ineffective in the management of bradykinin-mediated angioedema. Recent advancements in the understanding of angioedema have yielded pharmacologic treatment options for hereditary angioedema, a rare hereditary form of bradykinin-mediated angioedema. These novel therapies include a kallikrein inhibitor (ecallantide) and a bradykinin β2 receptor antagonist (icatibant). The physician's ability to distinguish between these types of angioedema is critical in optimizing outcomes in the acute care setting with appropriate treatment. This article reviews the pathophysiologic mechanisms, clinical presentations, and diagnostic laboratory evaluation of angioedema, along with acute management strategies for attacks.
Figures
References
-
- Winters M. Clinical practice guideline: initial evaluation and management of patients presenting with acute urticaria or angioedema. American Academy of Emergency Medicine Web site. http://www.aaem.org/em-resources/position-statements/2006/clinical-pract.... Updated July 10, 2006. Accessed September 14, 2012.
-
- Kaplan AP, Ausiello DA. In: Cecil Medicine. 23. Goldman L, editor. Saunders, Philadelphia; 2008. Anaphylaxis; pp. 1450–1452.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
