

The impact of systemic fungal infection in patients with perforated oesophagus
- PMID: 23131229
- PMCID: PMC3954285
- DOI: 10.1308/003588412X13373405388095
The impact of systemic fungal infection in patients with perforated oesophagus
Abstract
Introduction: Perforated oesophagus is a surgical emergency with significant morbidity and mortality. Systemic fungal infection represents a poor response to the magnitude of the insult, which adds significantly to the risk of morbidity and mortality in these patients. We reviewed our experience with this group of patients over a six-year period in a tertiary referral centre.
Methods: A retrospective clinical review was conducted of patients who were admitted following a ruptured oesophagus over a period of six years (January 2002 - January 2008).
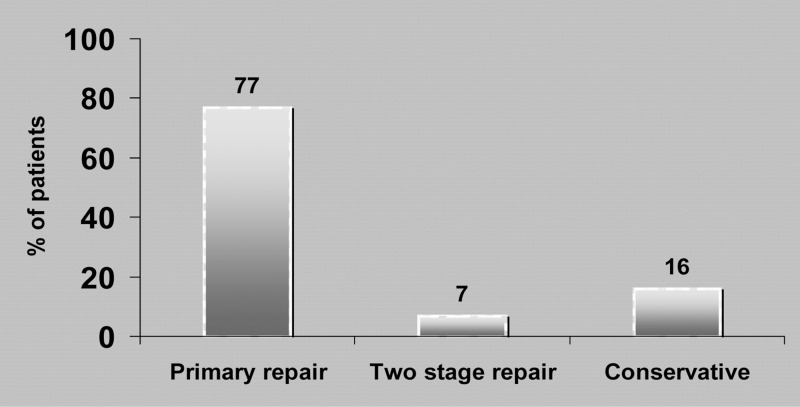
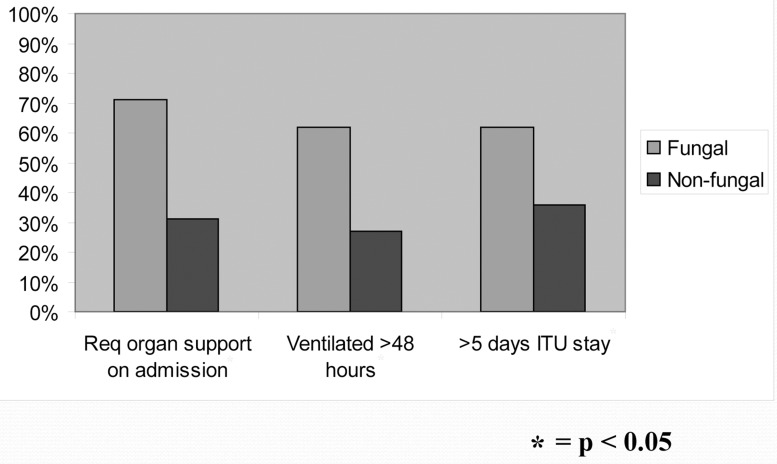
Results: We had 27 admissions (18 men and 9 women) following an isolated perforated oesophagus to our unit. The median patient age was 65 years (range: 22-87 years). The majority (n=24, 89%) presented with spontaneous perforations (Boerhaave's syndrome) and three (11%) were iatrogenic. Fungal organisms, predominantly Candida albicans, were positively cultured in pleural or blood samples in 16 (59%) of the 27 patients. Fourteen patients grew yeasts within the first seven days while two showed a delayed growth after ten days. Overall mortality was 5 out of 27 patients (19%). There was no mortality among the group that did not grow yeasts in their blood/pleural fluid while mortality was 31% (5/16) in the group with systemic fungal infection (p<0.001). A positive fungal culture was also associated with increase ventilation time, intensive care unit stay and inpatient hospital stay but not an increased rate of complications.
Conclusions: Systemic fungal infection in patients with a ruptured oesophagus affects a significant proportion of these patients and carries a poor prognosis despite advanced critical care interventions. It may represent a general marker of poor host response to a major insult but can add to mortality and morbidity. It is worth considering adding antifungal therapy empirically at an early stage to antimicrobials in patients with an established diagnosis of a perforated oesophagus.
Figures
Similar articles
-
The influence of the 'golden 24-h rule' on the prognosis of oesophageal perforation in the modern era.Eur J Cardiothorac Surg. 2010 Aug;38(2):216-22. doi: 10.1016/j.ejcts.2010.01.030. Epub 2010 Mar 20. Eur J Cardiothorac Surg. 2010. PMID: 20304664
-
Association of fungal infection and increased mortality in liver transplant recipients.Am J Surg. 2000 May;179(5):426-30. doi: 10.1016/s0002-9610(00)00366-4. Am J Surg. 2000. PMID: 10930495
-
[Complicated course of oesophageal perforations because of fungal infections].Mycoses. 2005;48 Suppl 1:41-5. doi: 10.1111/j.1439-0507.2005.01110.x. Mycoses. 2005. PMID: 15826286 German.
-
Role of Empiric Anti-Fungal Therapy in the Treatment of Perforated Peptic Ulcer Disease: Review of the Evidence and Future Directions.Surg Infect (Larchmt). 2019 Dec;20(8):593-600. doi: 10.1089/sur.2019.062. Epub 2019 Jun 12. Surg Infect (Larchmt). 2019. PMID: 31188069
-
Management of mycoses in surgical patients -- review of the literature.Eur J Med Res. 2002 May 31;7(5):200-26. Eur J Med Res. 2002. PMID: 12069912 Review.
Cited by
-
Not the Yeast of Our Worries: A Case of Amphetamine-Induced Esophagitis.J Brown Hosp Med. 2024 Jul 1;3(3):119029. doi: 10.56305/001c.119029. eCollection 2024. J Brown Hosp Med. 2024. PMID: 40026400 Free PMC article.
-
[Perforations near the cardia in benign diseases].Chirurg. 2014 Dec;85(12):1064-72. doi: 10.1007/s00104-014-2805-z. Chirurg. 2014. PMID: 25488114 Review. German.
-
Endoscopic Management of Esophageal Cancer.Cancers (Basel). 2022 Jul 22;14(15):3583. doi: 10.3390/cancers14153583. Cancers (Basel). 2022. PMID: 35892840 Free PMC article. Review.
-
Empiric Antimicrobial Treatment of Anastomotic Leakage after Esophageal Resection: The Most Commonly Used Antimicrobial Regimens in the Netherlands and an Antimicrobial Treatment Recommendation Based on a Single-Center Population.Dig Surg. 2025;42(2):68-76. doi: 10.1159/000545046. Epub 2025 Mar 5. Dig Surg. 2025. PMID: 40043696 Free PMC article.
-
Managing Acute Esophageal Necrosis Secondary to Diabetic Ketoacidosis in a Rural Centre: A Case Report and Proposed Algorithm for Management.Clin Case Rep. 2025 Feb 26;13(3):e70238. doi: 10.1002/ccr3.70238. eCollection 2025 Mar. Clin Case Rep. 2025. PMID: 40018430 Free PMC article.
References
-
- Brinster CJ, Singhal S, Lee Let al.Evolving options in the management of esophageal perforation. Ann Thorac Surg 2004; 77: 1,475–1,483 - PubMed
-
- Andersen LI, Frederiksen HJ, Appleyard M. Prevalence of esophageal Candida colonization in a Danish population: special reference to esophageal symptoms, benign esophageal disorders, and pulmonary disease. J Infect Dis 1992; 165: 389–392 - PubMed
-
- Dean DA, Burchard KW.Surgical perspective on invasive Candida infections. World J Surg 1998; 22: 127–134 - PubMed
-
- Calderone RA, Fonzi WA. Virulence factors of Candida albicans. Trends Microbiol 2001; 9: 327–335 - PubMed
-
- Jarvis WR. Epidemiology of nosocomial fungal infections, with emphasis on Candida species. Clin Infect Dis 1995; 20: 1,526–1,530 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical