

Neuroinflammatory imaging biomarkers: relevance to multiple sclerosis and its therapy
- PMID: 23132327
- PMCID: PMC3557362
- DOI: 10.1007/s13311-012-0155-4
Neuroinflammatory imaging biomarkers: relevance to multiple sclerosis and its therapy
Abstract
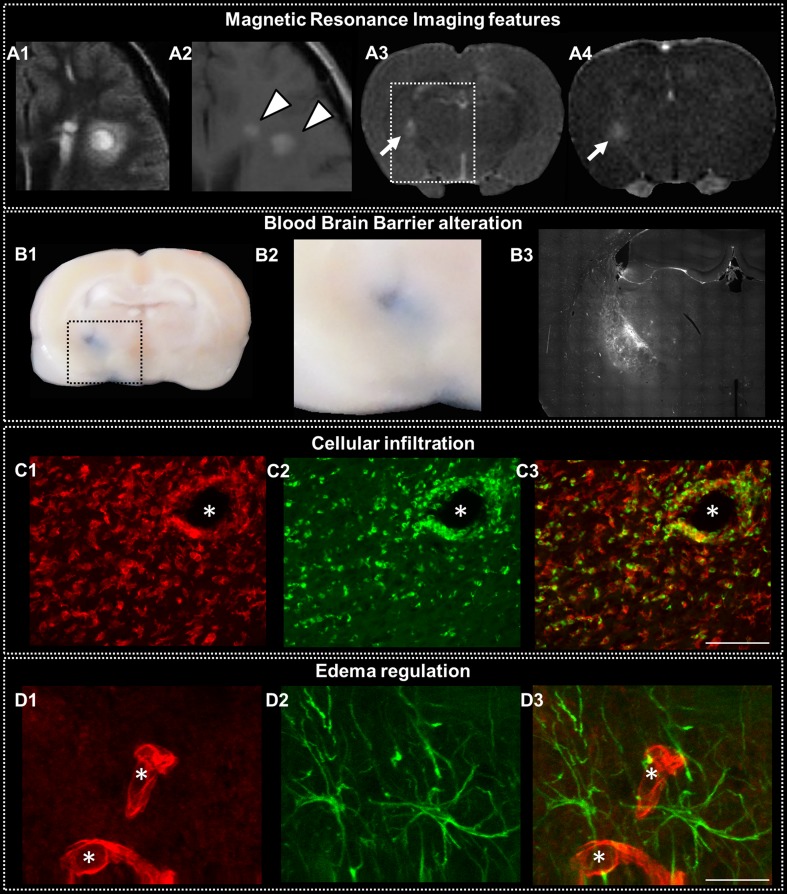
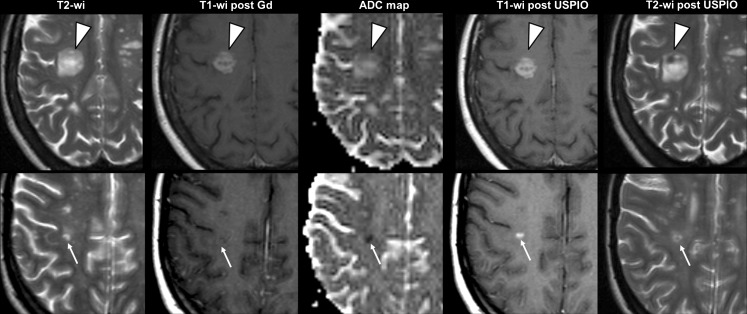
Magnetic resonance imaging is an established tool in the management of multiple sclerosis (MS). Loss of blood brain barrier integrity assessed by gadolinium (Gd) enhancement is the current standard marker of MS activity. To explore the complex cascade of the inflammatory events, other magnetic resonance imaging, but also positron emission tomographic markers reviewed in this article are being developed to address active neuroinflammation with increased sensitivity and specificity. Alternative magnetic resonance contrast agents, positron emission tomographic tracers and imaging techniques could be more sensitive than Gd to early blood brain barrier alteration, and they could assess the inflammatory cell recruitment and/or the associated edema accumulation. These markers of active neuroinflammation, although some of them are limited to experimental studies, could find great relevance to complete Gd information and thereby increase our understanding of acute lesion pathophysiology and its noninvasive follow-up, especially to monitor treatment efficacy. Furthermore, such accurate markers of inflammation combined with those of neurodegeneration hold promise to provide a more complete picture of MS, which will be of great benefit for future therapeutic strategies.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
