

Concomitant oral tyrosine kinase inhibitors and bisphosphonates in advanced renal cell carcinoma with bone metastases
- PMID: 23132391
- PMCID: PMC3493858
- DOI: 10.1038/bjc.2012.385
Concomitant oral tyrosine kinase inhibitors and bisphosphonates in advanced renal cell carcinoma with bone metastases
Abstract
Background: The presence of bone metastases in patients with metastatic renal cell carcinoma treated with oral tyrosine kinase inhibitors (TKIs) is associated with poorer outcome as compared with patients without bone involvement. Concomitant bisphosphonates could probably improve outcomes but also induce osteonecrosis of the jaw (ONJ).
Methods: Retrospective study on all the renal cell carcinoma patients with bone metastases treated with sunitinib or sorafenib between November 2005 and June 2012 at the University Hospitals Leuven and AZ Groeninge in Kortrijk.
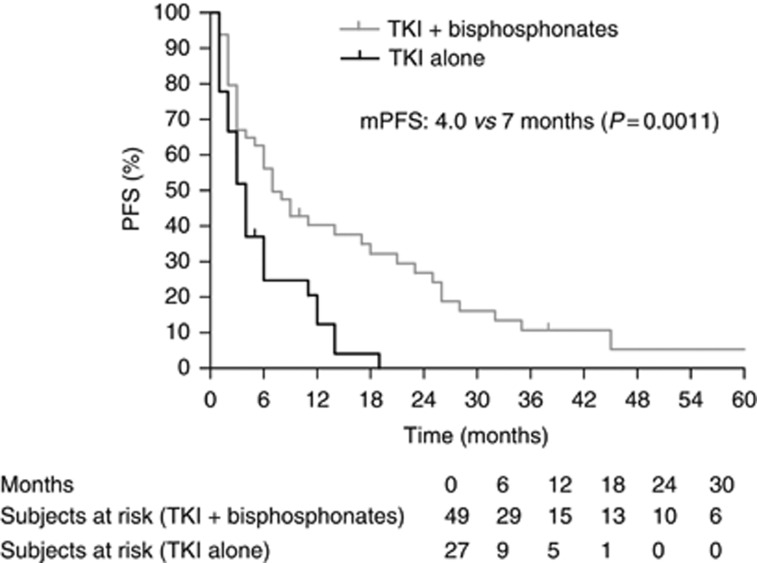
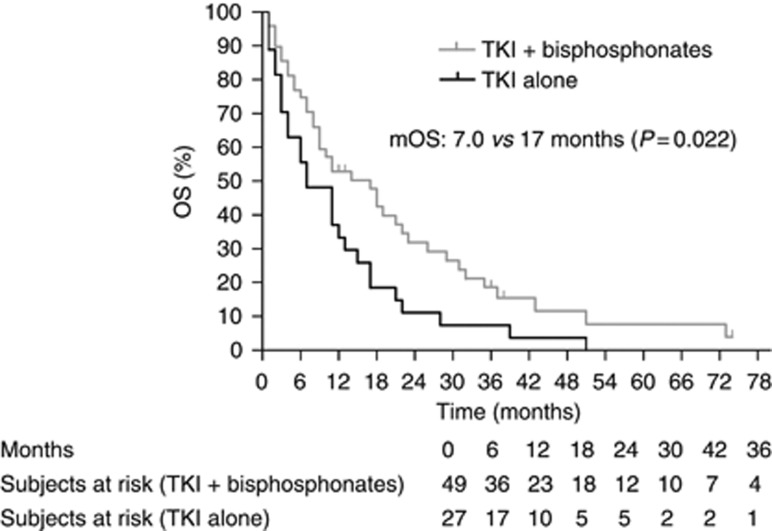
Results: Seventy-six patients were included in the outcome analysis: 49 treated with concomitant bisphosphonates, 27 with TKI alone. Both groups were well balanced in terms of prognostic and predictive markers. Response rate (38% vs 16% partial responses, P=0.028), median progression-free survival (7.0 vs 4.0 months, P=0.0011) and median overall survival (17.0 vs 7.0 months, P=0.022) were significantly better in patients receiving bisphosphonates. The incidence of ONJ was 10% in patients treated with TKI and bisphosphonates.
Conclusion: Concomitant use of bisphosphonates and TKI in renal cell carcinoma patients with bone involvement probably improves treatment efficacy, to be confirmed by prospective studies, but is associated with a high incidence of ONJ.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Prognostic significance of bone metastases and bisphosphonate therapy in patients with renal cell carcinoma.Eur Urol. 2014 Sep;66(3):502-9. doi: 10.1016/j.eururo.2014.02.040. Epub 2014 Feb 26. Eur Urol. 2014. PMID: 24613250 Free PMC article.
-
Bisphosphonates combined with sunitinib may improve the response rate, progression free survival and overall survival of patients with bone metastases from renal cell carcinoma.Eur J Cancer. 2012 May;48(7):1031-7. doi: 10.1016/j.ejca.2012.02.050. Epub 2012 Mar 10. Eur J Cancer. 2012. PMID: 22409947
-
Prolonged exposure to tyrosine kinase inhibitors or early use of everolimus in metastatic renal cell carcinoma: are the two options alike?Med Oncol. 2013;30(2):578. doi: 10.1007/s12032-013-0578-8. Epub 2013 Apr 24. Med Oncol. 2013. PMID: 23613183
-
Bisphosphonates and vascular endothelial growth factor-targeted drugs in the treatment of patients with renal cell carcinoma metastatic to bone.Anticancer Drugs. 2013 Jun;24(5):431-40. doi: 10.1097/CAD.0b013e328360335f. Anticancer Drugs. 2013. PMID: 23511427 Review.
-
Osteonecrosis of the Jaw in Patients With Metastatic Renal Cell Cancer Treated With Bisphosphonates and Targeted Agents: Results of an Italian Multicenter Study and Review of the Literature.Clin Genitourin Cancer. 2015 Aug;13(4):287-294. doi: 10.1016/j.clgc.2014.12.002. Epub 2014 Dec 9. Clin Genitourin Cancer. 2015. PMID: 25586958 Review.
Cited by
-
Medication-Related Osteonecrosis of the Jaw in Patients Treated Concurrently with Antiresorptive and Antiangiogenic Agents: Systematic Review and Meta-Analysis.J Immunother Precis Oncol. 2021 Sep 30;4(4):196-207. doi: 10.36401/JIPO-21-14. eCollection 2021 Nov. J Immunother Precis Oncol. 2021. PMID: 35665023 Free PMC article. Review.
-
Mechanisms Underlying Medication-Related Osteonecrosis of the Jaw.Oral Dis. 2025 Apr;31(4):1073-1083. doi: 10.1111/odi.15198. Epub 2024 Nov 18. Oral Dis. 2025. PMID: 39552606 Free PMC article. Review.
-
Osteonecrosis of the jaw (ONJ) in renal cell cancer patients after treatment including zoledronic acid or denosumab.Support Care Cancer. 2014 Jul;22(7):1737-8. doi: 10.1007/s00520-014-2159-6. Epub 2014 Feb 26. Support Care Cancer. 2014. PMID: 24570104 No abstract available.
-
Zoledronic acid in genitourinary cancer.Clin Transl Oncol. 2013 Nov;15(11):871-8. doi: 10.1007/s12094-013-1033-1. Epub 2013 Apr 25. Clin Transl Oncol. 2013. PMID: 23615978 Review.
-
MicroRNAs Possibly Involved in the Development of Bone Metastasis in Clear-Cell Renal Cell Carcinoma.Cancers (Basel). 2021 Mar 28;13(7):1554. doi: 10.3390/cancers13071554. Cancers (Basel). 2021. PMID: 33800656 Free PMC article.
References
-
- Ayllon J, Launay-Vacher V, Medioni J, Cros C, Spano JP, Oudard S (2009) Osteonecrosis of the jaw under bisphosphonate and antiangiogenic therapies: cumulative toxicity profile? Ann Oncol 20(3): 600–601 - PubMed
-
- Bamias A, Kastritis E, Bamia C, Moulopoulos LA, Melakopoulos I, Bozas G, Koutsoukou V, Gika D, Anagnostopoulos A, Papadimitriou C, Terpos E, Dimopoulos MA (2005) Osteonecrosis of the jaw in cancer after treatment with bisphosphonates: incidence and risk factors. J Clin Oncol 23(34): 8580–8587 - PubMed
-
- Beuselinck B, Oudard S, Rixe O, Wolter P, Blesius A, Ayllon J, Elaidi R, Schöffski P, Barrascout E, Morel A, Escudier B, Lang H, Zucman-Rossi J, Medioni J (2011) ‘Negative impact of bone metastasis on outcome in clear cell renal cell carcinoma treated with sunitinib’. Ann Oncol 22(4): 794–800 - PubMed
-
- Bozas G, Allgar V, Greenwood G, Maraveyas A (2011) Osteonecrosis of the jaw in patients treated with sunitinib and zoledronic acid. J Clin Oncol 29(Suppl): abstract e15116
-
- Christodoulou C, Pervena A, Klouvas G, Galani E, Falagas ME, Tsakalos G, Visvikis A, Nikolakopoulou A, Acholos V, Karapanagiotidis G, Batziou E, Skarlos DV (2009) Combination of bisphosphonates and antiangiogenic factors induces osteonecrosis of the jaw more frequently than bisphosphonates alone. Oncology 76(3): 209–211 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
