

Conceptual, methodological, and ethical problems in communicating uncertainty in clinical evidence
- PMID: 23132891
- PMCID: PMC4238424
- DOI: 10.1177/1077558712459361
Conceptual, methodological, and ethical problems in communicating uncertainty in clinical evidence
Abstract
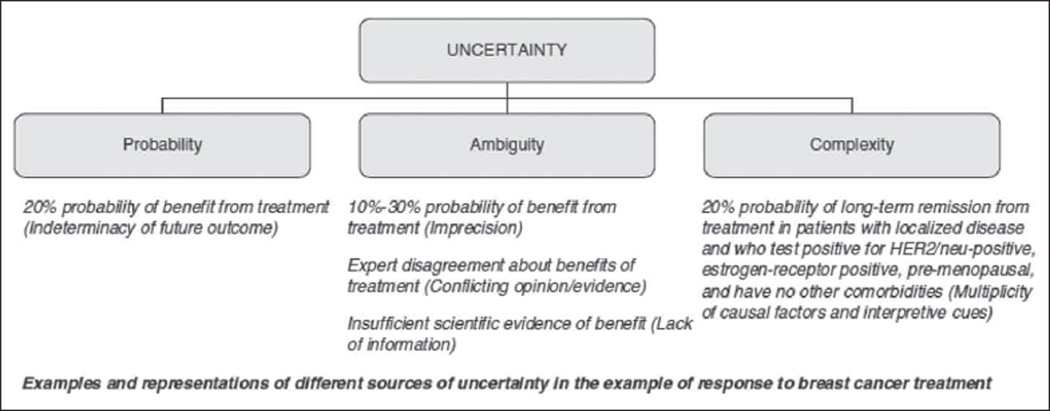
The communication of uncertainty in clinical evidence is an important endeavor that poses difficult conceptual, methodological, and ethical problems. Conceptual problems include logical paradoxes in the meaning of probability and "ambiguity"--second-order uncertainty arising from the lack of reliability, credibility, or adequacy of probability information. Methodological problems include questions about optimal methods for representing fundamental uncertainties and for communicating these uncertainties in clinical practice. Ethical problems include questions about whether communicating uncertainty enhances or diminishes patient autonomy and produces net benefits or harms. This article reviews the limited but growing literature on these problems and efforts to address them and identifies key areas of focus for future research. It is argued that the critical need moving forward is for greater conceptual clarity and consistent representational methods that make the meaning of various uncertainties understandable, and for clinical interventions to support patients in coping with uncertainty in decision making.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Akl EA, Guyatt GH, Irani J, Feldstein D, Wasi P, Shaw E, Schunemann HJ. “Might” or “suggest”? No wording approach was clearly superior in conveying the strength of recommendation. Journal of Clinical Epidemiology. 2012;65:268–275. - PubMed
-
- Asch DA, Hershey JC. Why some health policies don’t make sense at the bedside. Annals of Internal Medicine. 1995;122:846–850. - PubMed
-
- Balshem H, Helfand M, Schunemann HJ, Oxman AD, Kunz R, Brozek J, Guyatt GH. GRADE guidelines: 3. Rating the quality of evidence. Journal of Clinical Epidemiology. 2011;64:401–406. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
