

Body weight changes and outpatient medical care utilisation: Results of the MONICA/KORA cohorts S3/F3 and S4/F4
- PMID: 23133503
- PMCID: PMC3488805
- DOI: 10.3205/psm000087
Body weight changes and outpatient medical care utilisation: Results of the MONICA/KORA cohorts S3/F3 and S4/F4
Abstract
Objectives: To test the effects of body weight maintenance, gain, and loss on health care utilisation in terms of outpatient visits to different kinds of physicians in the general adult population.
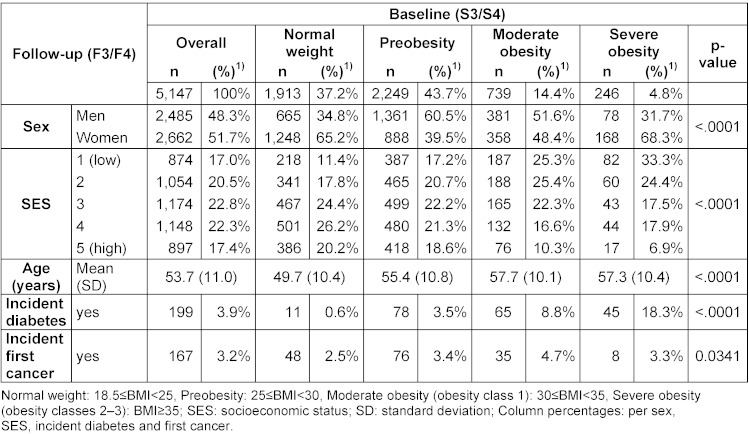
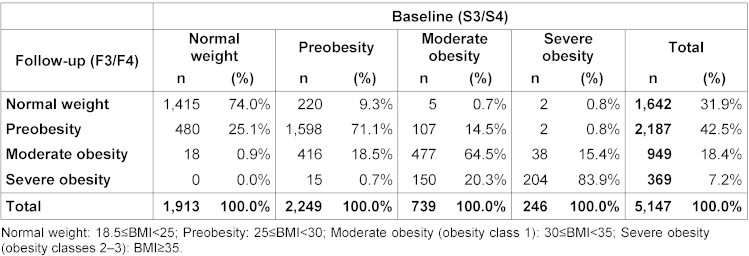
Methods: Self-reported utilisation data were collected within two population-based cohorts (baseline surveys: MONICA-S3 1994/95 and KORA-S4 1999/2001; follow-ups: KORA-F3 2004/05 and KORA-F4 2006/08) in the region of Augsburg, Germany, and were pooled for present purposes. N=5,147 adults (complete cases) aged 25 to 64 years at baseline participated. Number of visits to general practitioners (GPs), internists, and other specialists as well as the total number of physician visits at follow-up were compared across 10 groups defined by body mass index (BMI) category maintenance or change. Body weight and height were measured anthropometrically. Hierarchical generalized linear regression analyses with negative binomial distribution adjusted for sex, age, socioeconomic status (SES), survey, and the need factors incident diabetes and first cancer between baseline and follow-up were conducted.
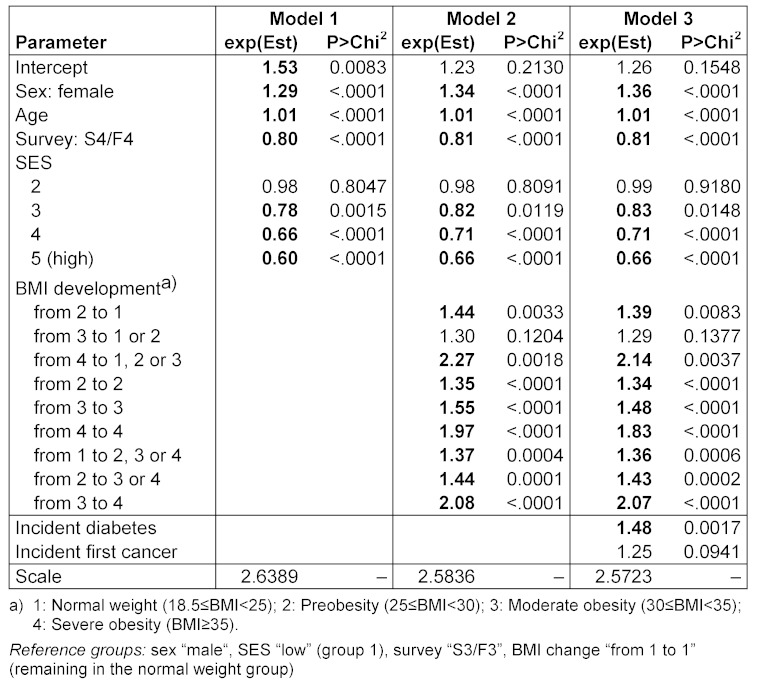
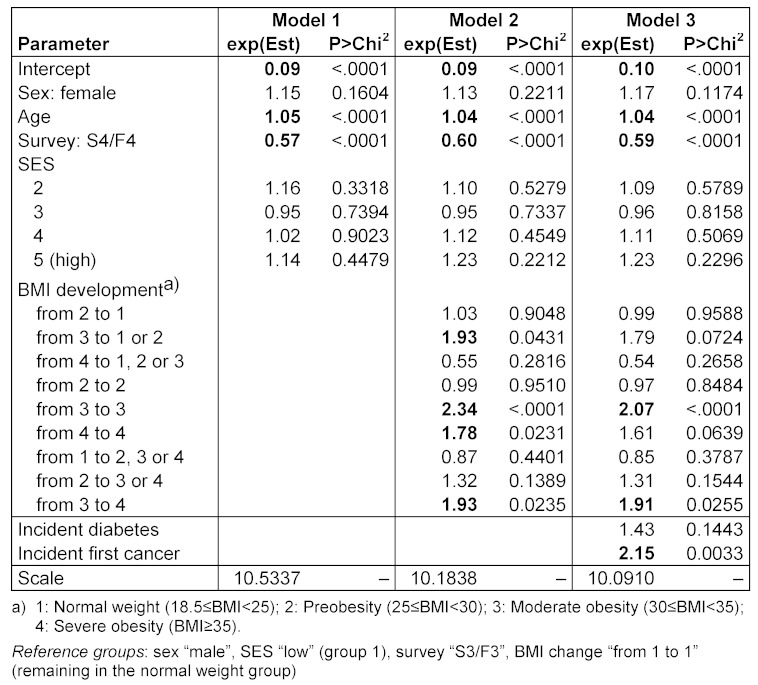
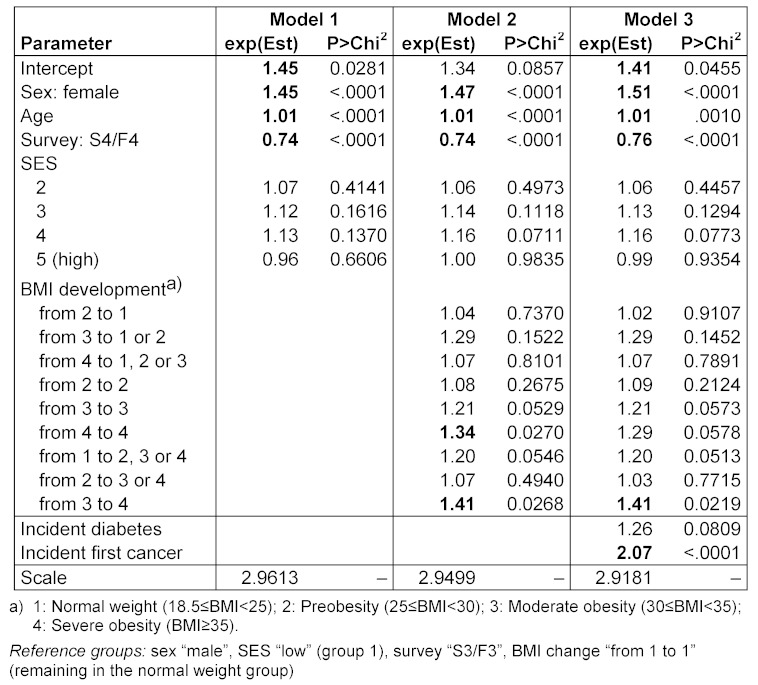
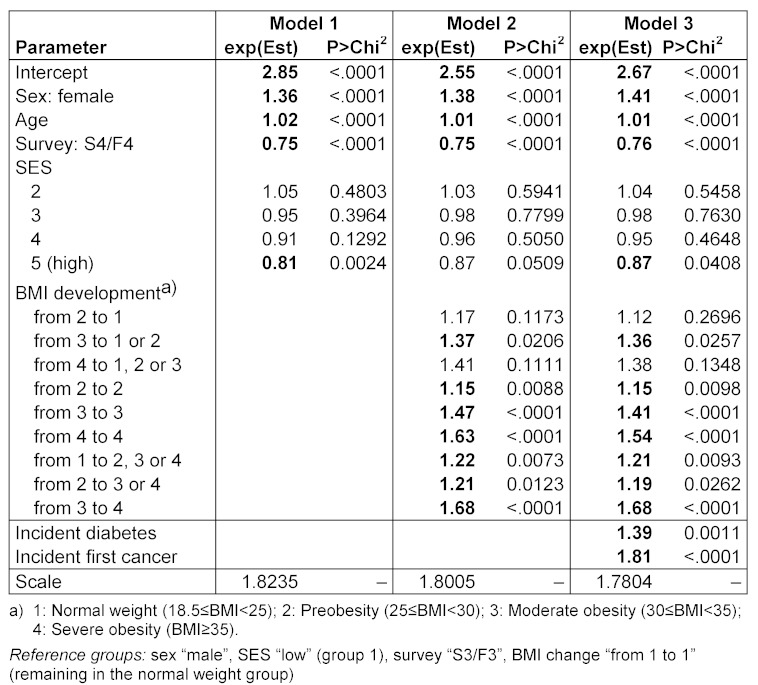
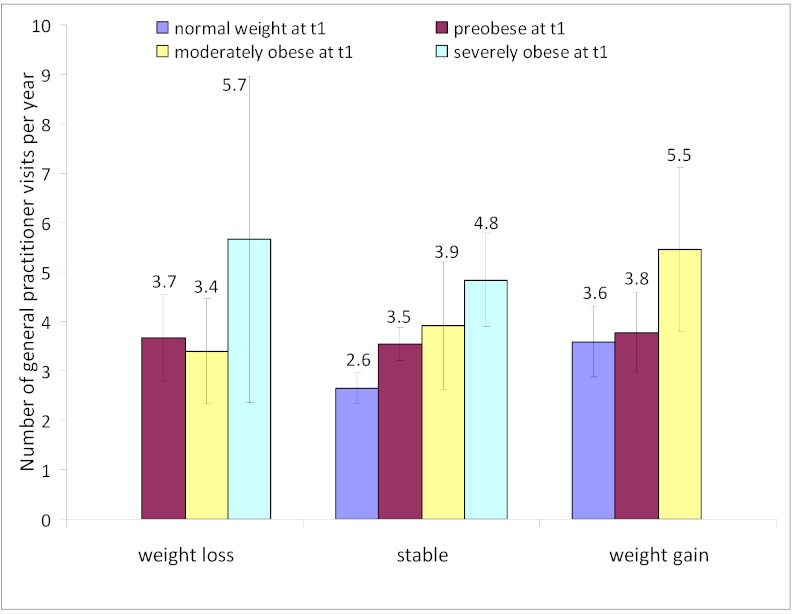
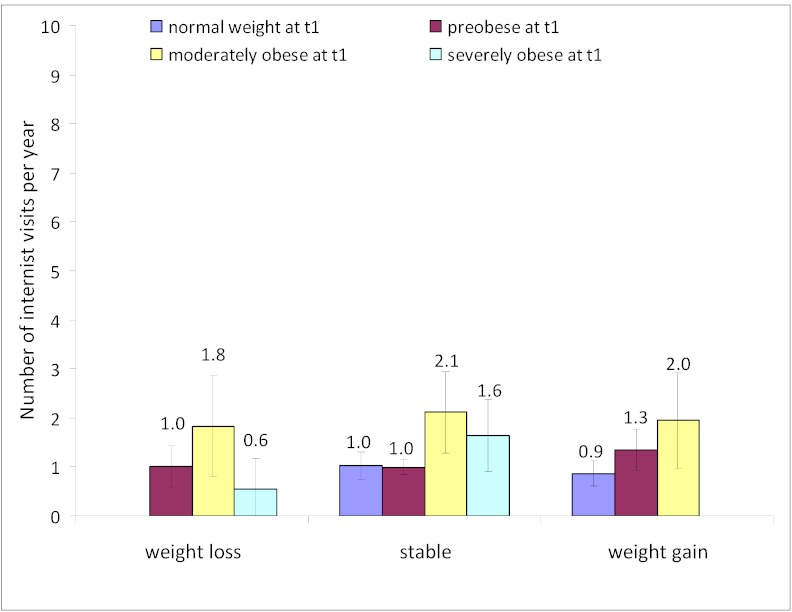
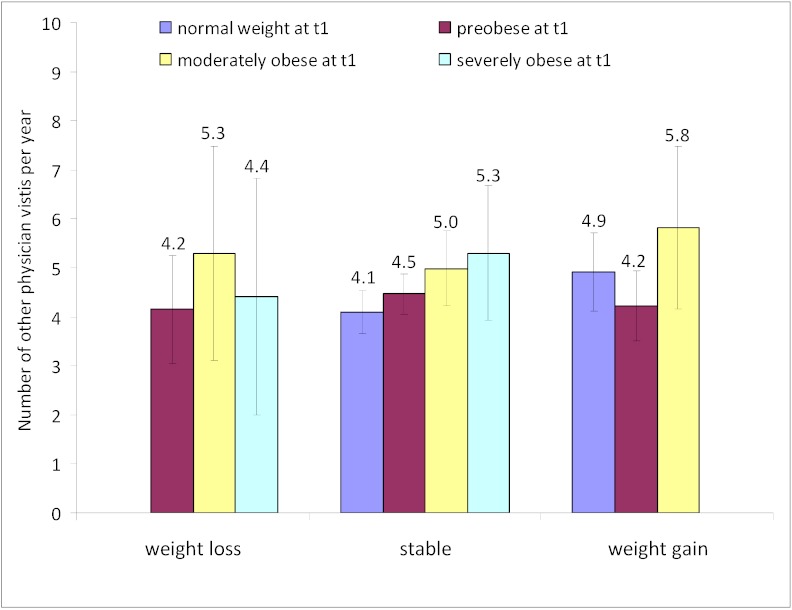
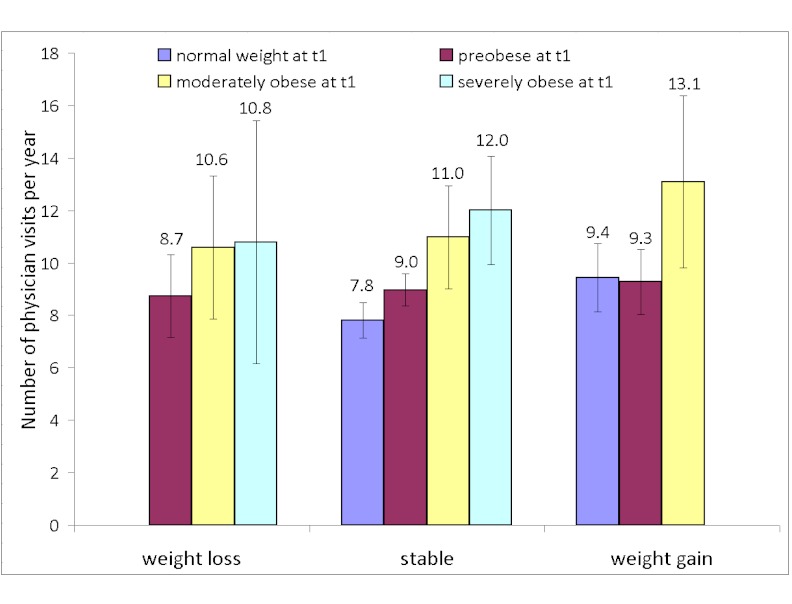
Results: In fully adjusted models, compared to the group of participants that maintained normal weight from baseline to follow-up, the following groups had significantly higher GP utilisation rates: weight gain from normal weight (+36%), weight loss from preobesity (+39%), maintained preobesity (+34%), weight gain after preobesity (+43%), maintained moderate obesity (+48%), weight gain from moderate obesity (+107%), weight loss from severe obesity (+114%), and maintained severe obesity (+83%). Regarding internists, those maintaining moderate obesity reported +107% more visits; those with weight gain from moderate obesity reported +91%. The latter group also had +41% more consultations with other physicians. Across all physicians, mean number of visits were estimated at 7.8 per year for maintained normal weight, 9 for maintained preobesity, 11 for maintained moderate obesity, and 12 for maintained severe obesity. Among those with weight loss, the mean number of visits were 8.7, 10.6 and 10.8 for baseline preobesity, moderate obesity, and severe obesity, respectively. Finally, those with weight gain from normal weight and preobesity reported 9.4 and 9.3 visits, respectively, and those with baseline moderate and follow-up severe obesity reported 13.1 visits (the most overall). Women reported higher GP and other physician utilisation. While all utilisation rates increased with age, GP utilisation was lower in middle to high SES groups.
Conclusion: Compared to maintained normal weight over a 7- to 10-year period, maintained overweight, weight gain and weight loss are associated with higher outpatient physician utilisation in adults, especially after baseline obesity. These effects only partly became insignificant after inclusion of incident diabetes or first cancer into the model. Future research should further elucidate the associations between weight development and health care utilisation by BMI status and the mechanisms underlying these associations.
Zielsetzung: Es werden Effekte der Erhaltung, Zunahme und des Verlusts von Körpergewicht auf Inanspruchnahme gesundheitsbezogener Versorgung im Sinne ambulanter Besuche bei verschiedenen Ärztegruppen in der erwachsenen Allgemeinbevölkerung untersucht.
Methodik: Selbstberichtete Inanspruchnahmedaten wurden im Rahmen zweier Populationskohorten (Baselinesurveys: MONICA-S3 1994/95 und KORA-S4 1999/2001; Follow-ups: KORA-F3 2004/05 und KORA-F4 2006/08) in der Region Augsburg erhoben und für die Analyse gepoolt. Zur Baseline nahmen N=5.147 Erwachsene (vollständige Fälle) im Alter von 25 bis 64 Jahren teil. Über 10 Gruppen, die nach Veränderungen oder dem Erhalt der Body Mass Index- (BMI-) Kategorie definiert wurden, wurde die Anzahl der Besuche bei Allgemeinmedizinern, Internisten und anderen Fachärzten sowie die Gesamtzahl der Arztbesuche beim Follow-up verglichen. Körpergröße und -gewicht wurden anthropometrisch gemessen. Es wurden hierarchische verallgemeinerte lineare Regressionsanalysen mit negativer Binomialverteilung durchgeführt und für Geschlecht, Alter, sozioökonomischen Status, Survey und für zwischen Baseline und Follow-up inzident aufgetretenen Diabetes und inzident aufgetretener erster Krebserkrankung als Bedarfsfaktoren adjustiert.
Ergebnisse: In den vollständig adjustierten Modellen hatten im Vergleich zur Gruppe der Teilnehmer, die von Baseline zum Follow-up normalgewichtig geblieben waren, folgende Gruppen eine signifikant höhere Inanspruchnahme von Allgemeinmedizinern: Gewichtszunahme nach Normalgewicht (+36%), Gewichtsabnahme nach Präadipositas (+39%), stabile Präadipositas (+34%), Gewichtszunahme nach Präadipositas (+43%), stabile moderate Adipositas (+48%), Gewichtszunahme nach moderater Adipositas (+107%), Gewichtsabnahme nach schwerer Adipositas (+114%) und stabile schwere Adipositas (+83%). Bezüglich Internisten berichteten Personen mit stabiler moderater Adipositas +107% mehr Besuche, und diejenigen mit einer Gewichtszunahme nach moderater Adipositas +91%. Diese letztere Gruppe zeichnete sich auch durch +41% mehr Besuche bei anderen Fachärzten aus. Über alle Ärzte hinweg wurde die mittlere Anzahl von Besuchen p. a. auf 7,8 bei stabilem Normalgewicht sowie auf 9 bei stabiler Präadipositas, 11 bei stabiler moderater Adipositas und 12 bei stabiler schwerer Adipositas geschätzt. Nach Gewichtsabnahme war die mittlere Anzahl der Besuche 8,7, 10,6 bzw. 10,8 bei initialer Präadipositas, moderater bzw. schwerer Adipositas. Diejenigen mit Gewichtszunahme nach Normalgewicht bzw. Präadipositas berichteten 9,4 bzw. 9,3 Besuche, während diejenigen mit initial moderater Adipositas und schwerer Adipositas zum Follow-up 13,1 Besuche (also insgesamt die meisten). Insgesamt berichteten Frauen über eine höhere Inanspruchnahme von Allgemeinmedizinern und anderen Fachärzten. Während alle Inanspruchnahmeparameter mit dem Alter zunahmen, war die Inanspruchnahme von Allgemeinmedizinern bei mittlerem bis höherem sozioökonomischem Status relativ gering.
Fazit: Über einen Beobachtungszeitraum von 7 bis 10 Jahren sind stabiles Übergewicht, Gewichtszunahme und Gewichtsabnahme bei Erwachsenen im Vergleich zu stabilem Normalgewicht mit einer erhöhten ambulanten Inanspruchnahme von Ärzten assoziiert. Dies gilt insbesondere bei initialer Adipositas. Die Effekte waren nur teilweise durch inzidenten Diabetes oder eine inzidente erste Krebserkrankung vermittelt. Zukünftige Studien sollten die Assoziationen zwischen Körpergewichtsentwicklung und der Inanspruchnahme von gesundheitsbezogener Versorgung nach BMI-Status sowie die zugrundeliegenden Mechanismen vertiefend analysieren.
Keywords: body mass index; body weight maintenance, gain, and loss; cohort studies; obesity; outpatient physician utilisation.
Figures
Similar articles
-
Future direct and indirect costs of obesity and the influence of gaining weight: results from the MONICA/KORA cohort studies, 1995-2005.Econ Hum Biol. 2012 Mar;10(2):127-38. doi: 10.1016/j.ehb.2011.08.008. Epub 2011 Sep 3. Econ Hum Biol. 2012. PMID: 21983232
-
Excess direct medical costs of severe obesity by socioeconomic status in German adults.Psychosoc Med. 2010 Apr 20;7:Doc01. doi: 10.3205/psm000063. Psychosoc Med. 2010. PMID: 20421952 Free PMC article.
-
[Direct medical costs of (severe) obesity: a bottom-up assessment of over- vs. normal-weight adults in the KORA-study region (Augsburg, Germany)].Gesundheitswesen. 2006 Feb;68(2):110-5. doi: 10.1055/s-2005-858994. Gesundheitswesen. 2006. PMID: 16482491 German.
-
Healthcare utilisation in overweight and obese children: a systematic review and meta-analysis.BMJ Open. 2020 Oct 8;10(10):e035676. doi: 10.1136/bmjopen-2019-035676. BMJ Open. 2020. PMID: 33033082 Free PMC article.
-
Association of fetuin-A with incident type 2 diabetes: results from the MONICA/KORA Augsburg study and a systematic meta-analysis.Eur J Endocrinol. 2018 Apr;178(4):389-398. doi: 10.1530/EJE-17-1053. Epub 2018 Feb 8. Eur J Endocrinol. 2018. PMID: 29439057
Cited by
-
Economic impacts of overweight and obesity: current and future estimates for eight countries.BMJ Glob Health. 2021 Oct;6(10):e006351. doi: 10.1136/bmjgh-2021-006351. BMJ Glob Health. 2021. PMID: 34737167 Free PMC article.
-
Specific Metabolic Markers Are Associated with Future Waist-Gaining Phenotype in Women.PLoS One. 2016 Jun 20;11(6):e0157733. doi: 10.1371/journal.pone.0157733. eCollection 2016. PLoS One. 2016. PMID: 27322650 Free PMC article.
-
Body Mass Index Trajectories and Healthcare Utilization in Young and Middle-aged Adults.Medicine (Baltimore). 2016 Jan;95(2):e2467. doi: 10.1097/MD.0000000000002467. Medicine (Baltimore). 2016. PMID: 26765446 Free PMC article.
-
Obesity and sickness absence: results from a longitudinal nationally representative sample from Germany.BMJ Open. 2018 Jun 6;8(6):e019839. doi: 10.1136/bmjopen-2017-019839. BMJ Open. 2018. PMID: 29880564 Free PMC article.
-
Impact of BMI and BMI change on future drug expenditures in adults: results from the MONICA/KORA cohort study.BMC Health Serv Res. 2013 Oct 19;13:424. doi: 10.1186/1472-6963-13-424. BMC Health Serv Res. 2013. PMID: 24139278 Free PMC article.
References
-
- WHO. Obesity: preventing and managing the global epidemic. Report of a WHO consultation. Geneva: WHO; 2000. - PubMed
-
- Popkin BM, Kim S, Rusev ER, Du S, Zizza C. Measuring the full economic costs of diet, physical activity and obesity-related chronic diseases. Obes Rev. 2006;7:271–293. doi: 10.1111/j.1467-789X.2006.00230.x. Available from: http://dx.doi.org/10.1111/j.1467-789X.2006.00230.x. - DOI - DOI - PubMed
-
- Misra A, Khurana L. Obesity and the metabolic syndrome in developing countries. J Clin Endocrinol Metab. 2008;93:S9–30. doi: 10.1210/jc.2008-1595. Available from: http://dx.doi.org/10.1210/jc.2008-1595. - DOI - DOI - PubMed
-
- Berghofer A, Pischon T, Reinhold T, Apovian CM, Sharma AM, Willich SN. Obesity prevalence from a European perspective: a systematic review. BMC Public Health. 2008;8:200. doi: 10.1186/1471-2458-8-200. Available from: http://dx.doi.org/10.1186/1471-2458-8-200. - DOI - DOI - PMC - PubMed
-
- von Ruesten A, Steffen A, Floegel A, van der A DL, Masala G, Tjønneland A, Halkjaer J, Palli D, Wareham NJ, Loos RJ, Sørensen TI, Boeing H. Trend in obesity prevalence in European adult cohort populations during follow-up since 1996 and their predictions to 2015. PLoS One. 2011;6:e27455. doi: 10.1371/journal.pone.0027455. Available from: http://dx.doi.org/10.1371/journal.pone.0027455. - DOI - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
