

The clinical efficacy of decompressive craniectomy in patients with an internal carotid artery territory infarction
- PMID: 23133715
- PMCID: PMC3488635
- DOI: 10.3340/jkns.2012.52.4.293
The clinical efficacy of decompressive craniectomy in patients with an internal carotid artery territory infarction
Abstract
Objective: To evaluate the surgical efficacy of and factors associated with decompressive craniectomy in patients with an internal carotid artery (ICA) territory infarction.
Methods: Seventeen patients (8 men and 9 women, average age 61.53 years, range 53-77 years) were treated by decompressive craniectomy for an ICA territory infarction at our institute. We retrospectively reviewed medical records, radiological findings, and National Institutes of Health Stroke Scale (NIHSS) at presentation and before surgery. Clinical outcomes were assessed using the Glasgow Outcome Scale (GOS).
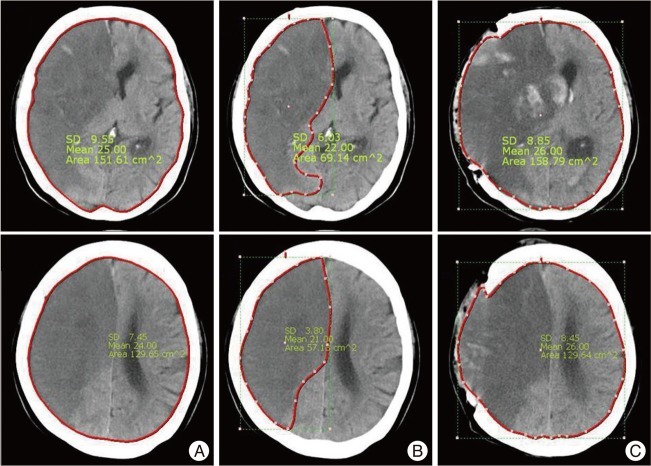
Results: Of the 17 patients, 15 (88.24%) achieved a poor outcome (Group A, GOS 1-3) and 2 (11.76%) a good outcome (Group B, GOS 4-5). The mortality rate at one month after surgery was 52.9%. Average preoperative NIHSS was 27.6±10.88% in group A and 10±4.24% in group B. Mean cerebral infarction fraction at the septum pellucidum level before surgery in group A and B were 33.67% and 23.72%, respectively. Mean preoperative NIHSS (p=0.019) and cerebral infarction fraction at the septum pellucidum level (p=0.017) were found to be significantly associated with a better outcome. However, no preexisting prognostic factor was found to be of statistical significance.
Conclusion: The rate of mortality after ICA territory infarction treatment is relatively high, despite positive evidence for surgical decompression, and most survivors experience severe disabilities. Our findings caution that careful consideration of prognostic factors is required when considering surgical treatment.
Keywords: Cerebral infarction; Decompressive craniectomy; Surgical efficacy.
Figures
References
-
- Bendszus M, Müllges W, Goldbrunner R, Weigand A, Solymosi L. Hemodynamic effects of decompressive craniotomy in MCA infarction : evaluation with perfusion CT. Eur Radiol. 2003;13:1895–1898. - PubMed
-
- Berrouschot J, Sterker M, Bettin S, Köster J, Schneider D. Mortality of space-occupying ('malignant') middle cerebral artery infarction under conservative intensive care. Intensive Care Med. 1998;24:620–623. - PubMed
-
- Carter BS, Ogilvy CS, Candia GJ, Rosas HD, Buonanno F. One-year outcome after decompressive surgery for massive nondominant hemispheric infarction. Neurosurgery. 1997;40:1168–1175. discussion 1175-1176. - PubMed
-
- Chen CC, Cho DY, Tsai SC. Outcome and prognostic factors of decompressive hemicraniectomy in malignant middle cerebral artery infarction. J Chin Med Assoc. 2007;70:56–60. - PubMed
-
- Cho TK, Cheong JH, Kim JH, Bak KH, Kim CH, Kim JM. Efficacy of the decompressive craniectomy for acute cerebral infarction : timing of surgical intervention and clinical prognostic factors. J Korean Neurosurg Soc. 2006;40:11–15.
LinkOut - more resources
Full Text Sources
Miscellaneous
