

Meningeal layers around anterior clinoid process as a delicate area in extradural anterior clinoidectomy : anatomical and clinical study
- PMID: 23133730
- PMCID: PMC3488650
- DOI: 10.3340/jkns.2012.52.4.391
Meningeal layers around anterior clinoid process as a delicate area in extradural anterior clinoidectomy : anatomical and clinical study
Abstract
Objective: Removal of the anterior clinoid process (ACP) is an essential process in the surgery of giant or complex aneurysms located near the proximal internal carotid artery or the distal basilar artery. An extradural clinoidectomy must be performed within the limits of the meningeal layers surrounding the ACP to prevent morbid complications. To identify the safest method of extradural exposure of the ACP, anatomical studies were done on cadaver heads.
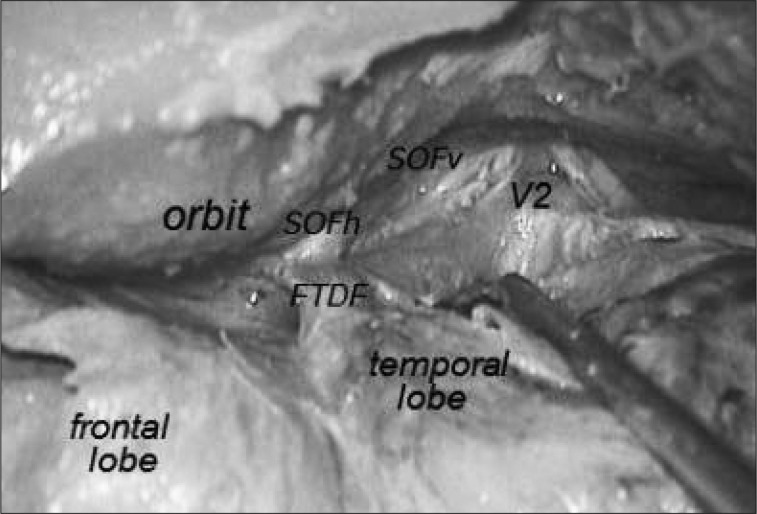
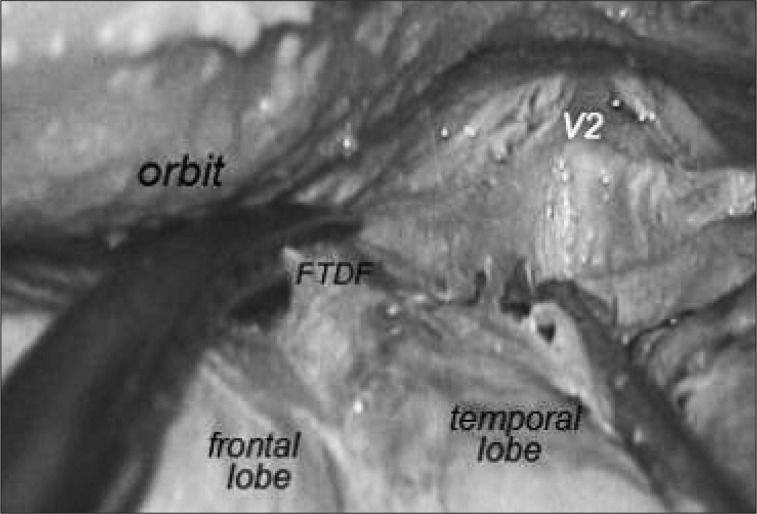
Methods: Anatomical dissections for extradural exposure of the ACP were performed on both sides of seven cadavers. Before dividing the frontotemporal dural fold (FTDF), we measured its length from the superomedial apex attached to the periorbita to the posterolateral apex which connects to the anterosuperior end of the cavernous sinus.
Results: The average length of the FTDF on cadaver dissections was 7 mm on the right side and 7.14 mm on the left side. Cranial nerves were usually exposed when cutting FTDF more than 7 mm of the FTDF.
Conclusion: The most delicate area in an extradural anterior clinoidectomy is the junction of the FTDF and the anterior triangular apex of the cavernous sinus. The FTDF must be cut from the anterior side of the triangle at the periorbital side rather than from the dural side. The length of the FTDF incision must not exceed 7 mm to avoid cranial nerve injury.
Keywords: Anatomical study; Extradural clinoidectomy; Frontotemporal dural fold; Superior orbital fissure.
Figures


Similar articles
-
An alternative extradural exposure to the anterior clinoid process: the superior orbital fissure as a surgical corridor.Neurosurgery. 2003 Jul;53(1):162-6; discussion 166-7. doi: 10.1227/01.neu.0000068866.22176.07. Neurosurgery. 2003. PMID: 12823885 Review.
-
Looking Beyond the Anterolateral Skull Base with Frontotemporal Dural Fold Unlocking and Extradural Clinoidectomy: A Series of 17 Cases Deciphering the Translation from a Cadaver to Real, and Real to Pathologically Distorted Anatomy.Neurol India. 2023 Mar-Apr;71(2):312-319. doi: 10.4103/0028-3886.375404. Neurol India. 2023. PMID: 37148059
-
Treading Toward Anterolateral Skull Base by Unlocking the Frontotemporal Dural Fold Along with Extradural Clinoidectomy: Translation from A Cadaver to Clinical Scenario.Neurol India. 2021 Jul-Aug;69(4):829-832. doi: 10.4103/0028-3886.325332. Neurol India. 2021. PMID: 34507396
-
Anatomical meningo-orbital band evaluation and clinical implications: a cadaveric dissection study.J Neurosurg Sci. 2022 Jun;66(3):215-219. doi: 10.23736/S0390-5616.19.04794-5. Epub 2019 Nov 13. J Neurosurg Sci. 2022. PMID: 31738027
-
Intra- and extradural anterior clinoidectomy: anatomy review and surgical technique step by step.Surg Radiol Anat. 2021 Aug;43(8):1291-1303. doi: 10.1007/s00276-021-02681-1. Epub 2021 Jan 25. Surg Radiol Anat. 2021. PMID: 33495868 Review.
Cited by
-
The Orbitomeningeal Band as a Way to Bloodless Transcavernous Dissection and Anterior Clinoidectomy.Asian J Neurosurg. 2018 Jul-Sep;13(3):943-945. doi: 10.4103/ajns.AJNS_198_16. Asian J Neurosurg. 2018. PMID: 30283589 Free PMC article.
-
Less Invasive Modified Extradural Temporopolar Approach for Paraclinoid Lesions: Operative Technique and Surgical Results in 80 Consecutive Patients.J Neurol Surg B Skull Base. 2018 Oct;79(Suppl 4):S347-S355. doi: 10.1055/s-0038-1654703. Epub 2018 May 25. J Neurol Surg B Skull Base. 2018. PMID: 30210989 Free PMC article.
-
Operative surgical nuances of modified extradural temporopolar approach with mini-peeling of dura propria based on cadaveric anatomical study of lateral cavernous structures.Surg Neurol Int. 2016 Jul 7;7(Suppl 16):S454-8. doi: 10.4103/2152-7806.185774. eCollection 2016. Surg Neurol Int. 2016. PMID: 27500005 Free PMC article.
-
The pterional approach and extradural anterior clinoidectomy to clip paraclinoid aneurysms.J Cerebrovasc Endovasc Neurosurg. 2013 Sep;15(3):260-6. doi: 10.7461/jcen.2013.15.3.260. Epub 2013 Sep 30. J Cerebrovasc Endovasc Neurosurg. 2013. PMID: 24167811 Free PMC article.
-
Ten Triangles around Cavernous Sinus for Surgical Approach, Described by Schematic Diagram and Three Dimensional Models with the Sectioned Images.J Korean Med Sci. 2016 Sep;31(9):1455-63. doi: 10.3346/jkms.2016.31.9.1455. J Korean Med Sci. 2016. PMID: 27510391 Free PMC article.
References
-
- Avci E, Bademci G, Ozturk A. Microsurgical landmarks for safe removal of anterior clinoid process. Minim Invasive Neurosurg. 2005;48:268–272. - PubMed
-
- Bayassi S. [Meningo-orbital fold (MOF) as a guiding point in extradural approach to the anterior clinoid process] Neurol Neurochir Pol. 2005;39:49–55. - PubMed
-
- Collignon F, Link M. Paraclinoid and cavernous sinus regions : measurement of critical structures relevant for surgical procedure. Clin Anat. 2005;18:3–9. - PubMed
-
- Coscarella E, Başkaya MK, Morcos JJ. An alternative extradural exposure to the anterior clinoid process : the superior orbital fissure as a surgical corridor. Neurosurgery. 2003;53:162–166. discussion 166-167. - PubMed
-
- Day AL. Aneurysms of the ophthalmic segment. A clinical and anatomical analysis. J Neurosurg. 1990;72:677–691. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
