

doi: 10.1155/2012/503254.
Epub 2012 Oct 24.
Bedside ultrasound in resuscitation and the rapid ultrasound in shock protocol
Affiliations
- PMID: 23133747
- PMCID: PMC3485910
- DOI: 10.1155/2012/503254
Item in Clipboard
Bedside ultrasound in resuscitation and the rapid ultrasound in shock protocol
Crit Care Res Pract.
2012.
Abstract
Assessment of hemodynamic status in a shock state remains a challenging issue in Emergency Medicine and Critical Care. As the use of invasive hemodynamic monitoring declines, bedside-focused ultrasound has become a valuable tool in the evaluation and management of patients in shock. No longer a means to simply evaluate organ anatomy, ultrasound has expanded to become a rapid and noninvasive method for the assessment of patient physiology. Clinicians caring for critical patients should strongly consider integrating ultrasound into their resuscitation pathways.
Figures
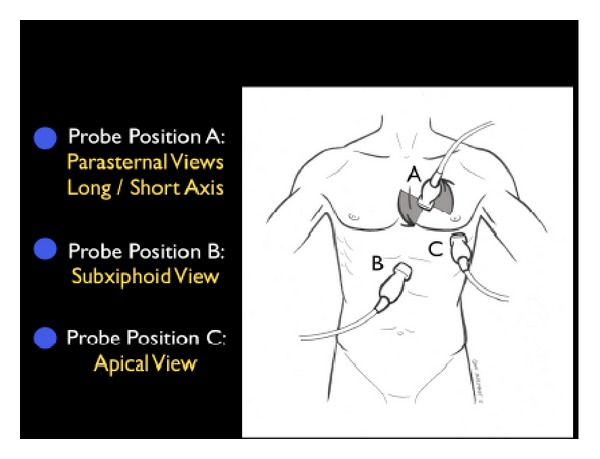
The RUSH exam. Step 1: Evaluation of “the pump”.
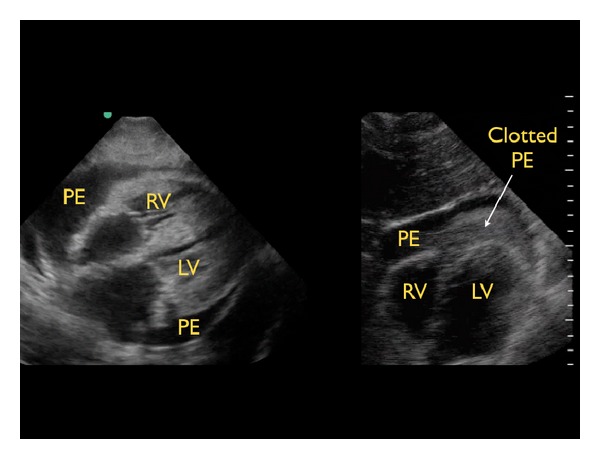
Types of pericardial effusions, subxiphoid cardiac view. Left image: typical effusion, right image: clotted effusion. RV: right ventricle, LV: left ventricle, PE: pericardial effusion.
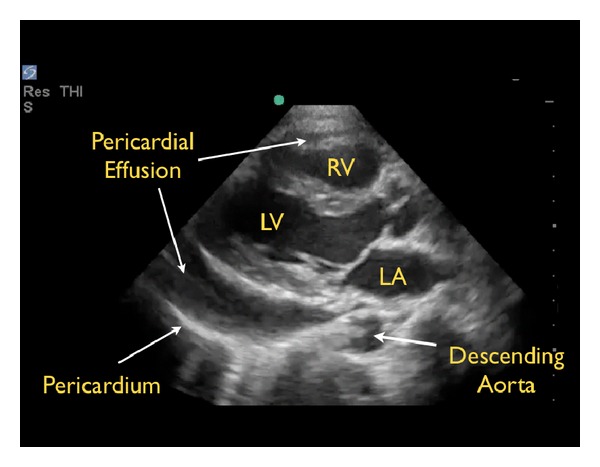
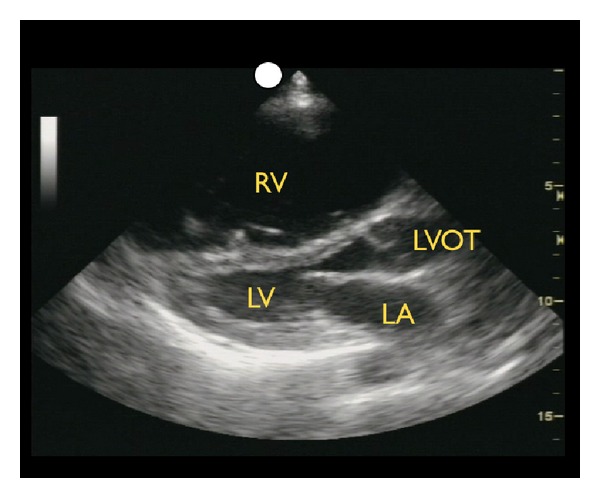
Pericardial effusion, parasternal long axis view. RV: right ventricle, LV: left ventricle, LA: left atrium.
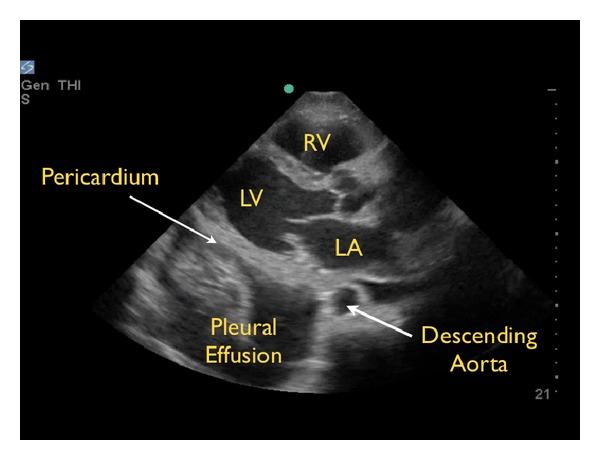
Pleural effusion, parasternal long axis view RV: right ventricle, LV: left ventricle, LA: left atrium.
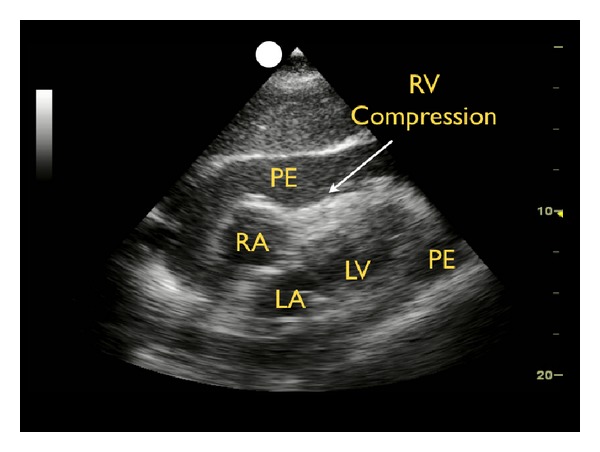
Cardiac tamponade, subxiphoid view. RV: right ventricle, RV: right atrium, LV: left ventricle, LA: left atrium, PE: pericardial effusion.
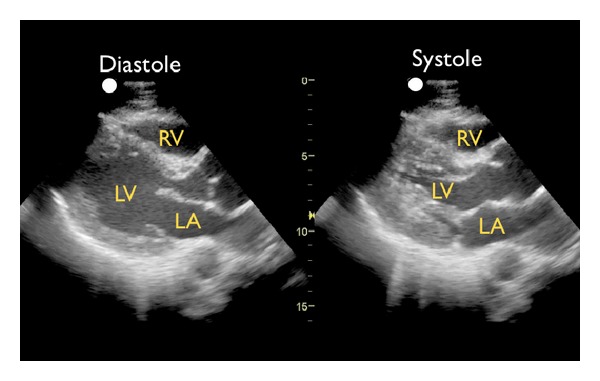
Good left ventricular contractility, parasternal long axis view. RV: right ventricle, LV: left ventricle, LA: left atrium.
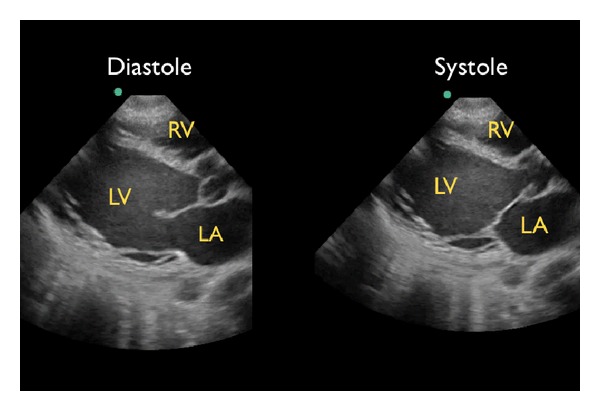
Poor left ventricular contractility, parasternal long axis view. RV: right ventricle, LV: left ventricle, LA: left atrium.
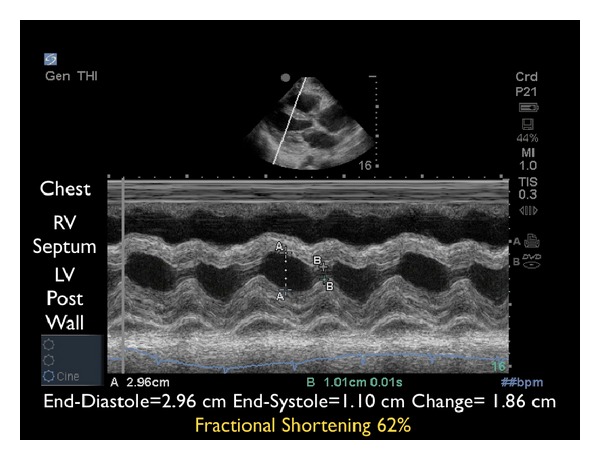
M-mode tracing demonstrating excellent contractility. RV: right ventricle, LV: left ventricle.
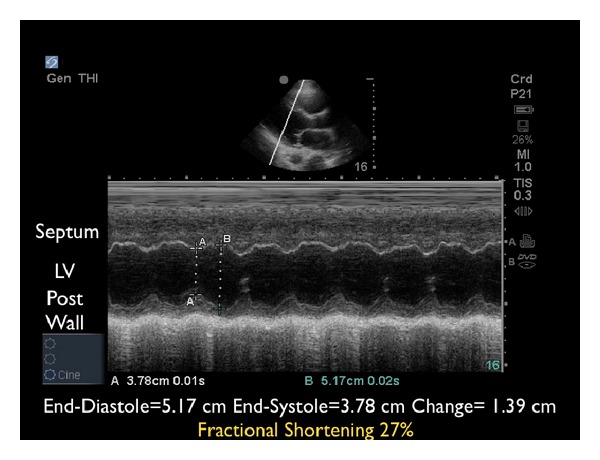
M-mode tracing demonstrating poor contractility. LV: left ventricle.
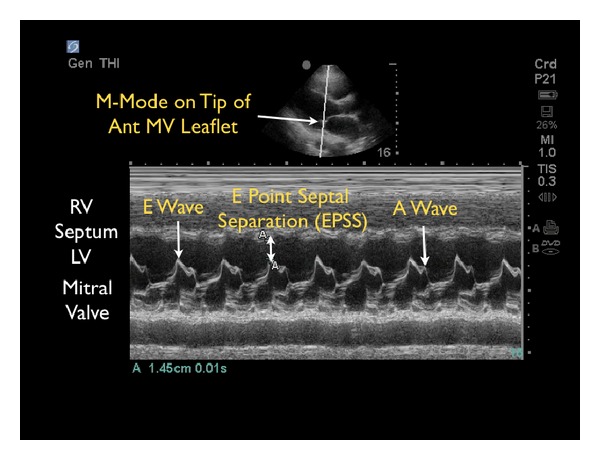
E-point septal separation with decreased contractility. M-mode Doppler tracing. RV: right ventricle, LV: left ventricle.
Right ventricular dilation, parasternal long axis view. RV: right ventricle, LA: left atrium, LV: left ventricle, LVOT: left ventricle outflow tract.
The RUSH exam. Step 2: Evaluation of “the tank”.
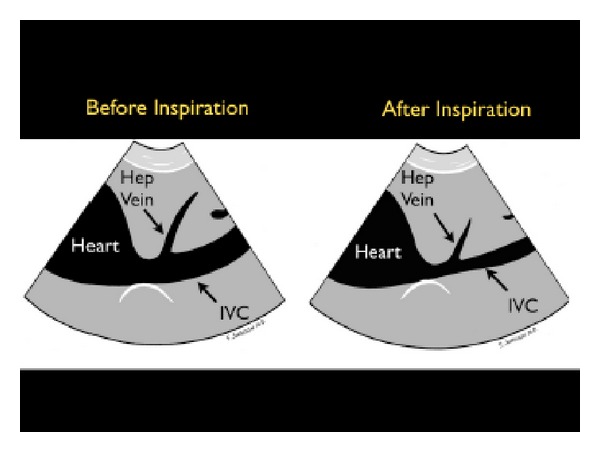
Collapsible inferior vena cava, long axis view.
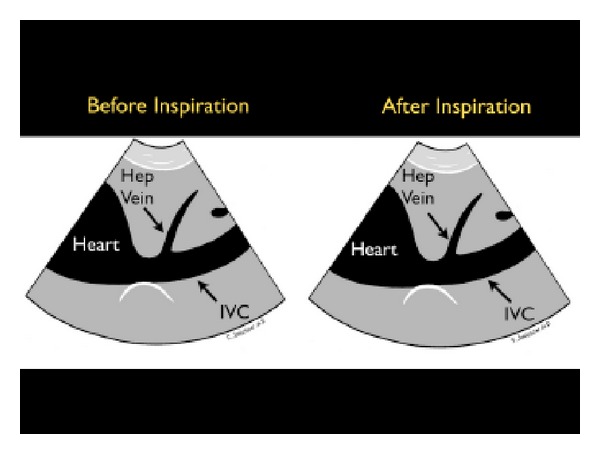
Inferior vena cava plethora, long axis view.
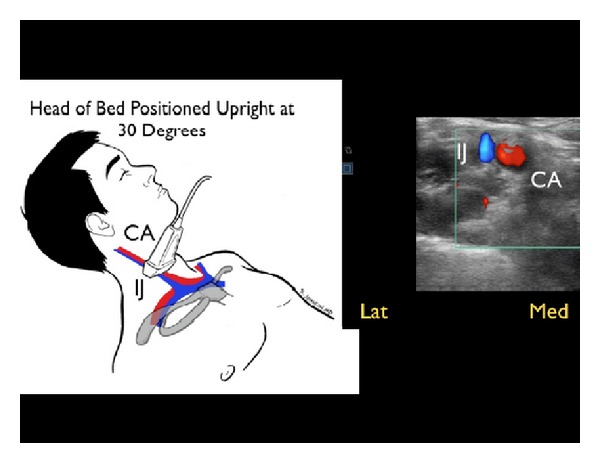
Small, collapsing internal jugular vein, short axis view. IJ: internal jugular vein, CA: carotid artery.
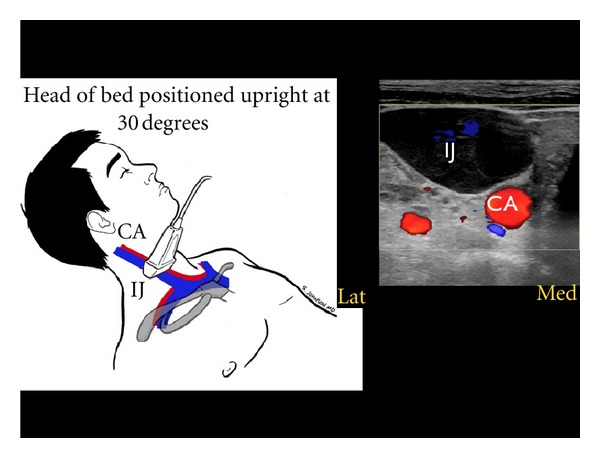
Large, distended internal jugular vein, short axis view. IJ: internal jugular vein, CA: carotid artery.
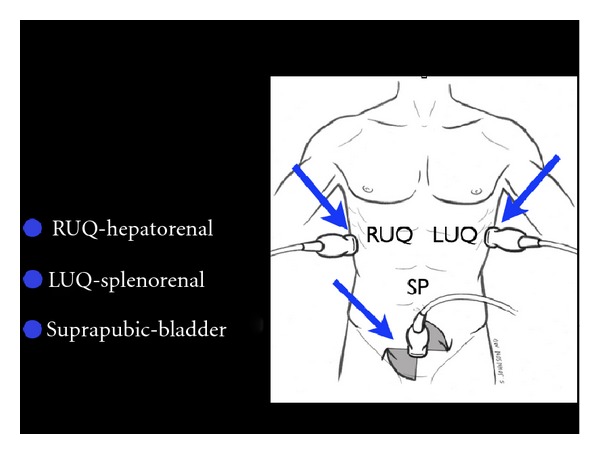
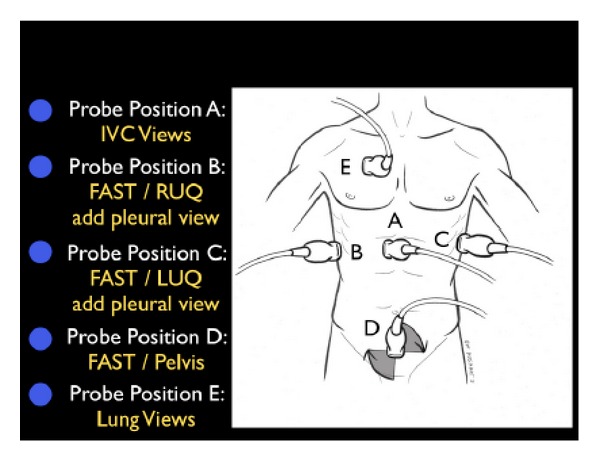
FAST exam.
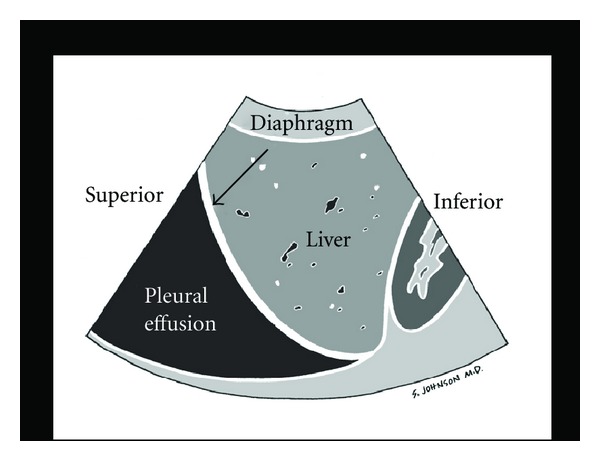
Pleural effusion.
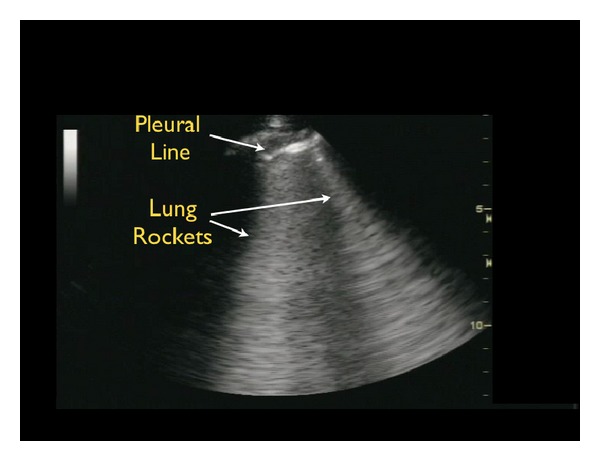
Pulmonary edema B-lines.
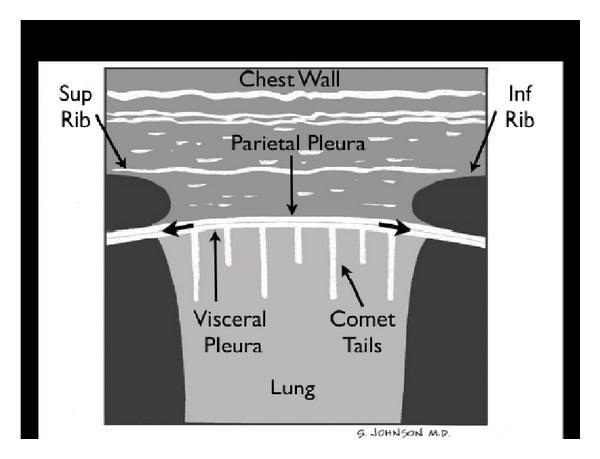
Normal lung.
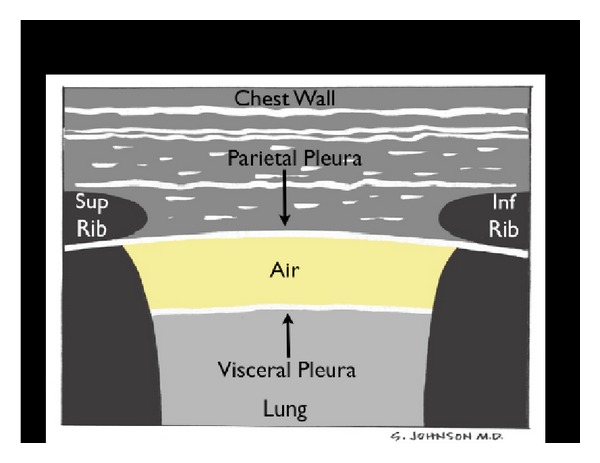
Pneumothorax.
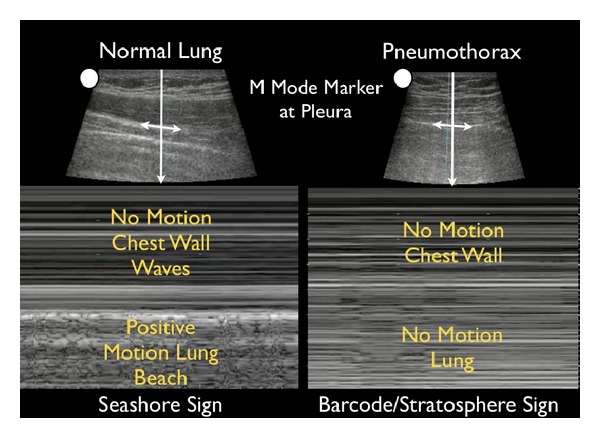
M-mode of normal lung versus pneumothorax.
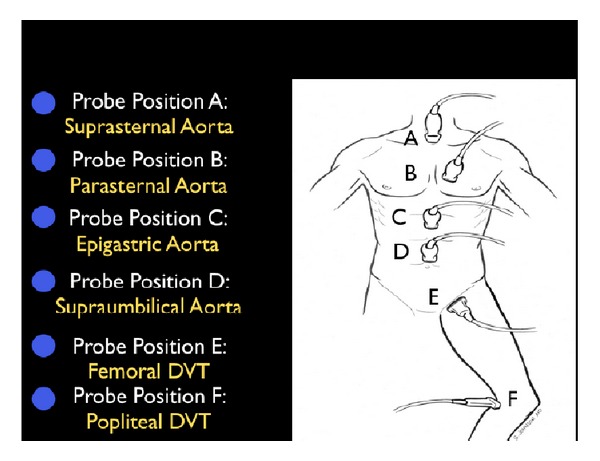
The RUSH exam. Step 3: Evaluation of “the pipes”.
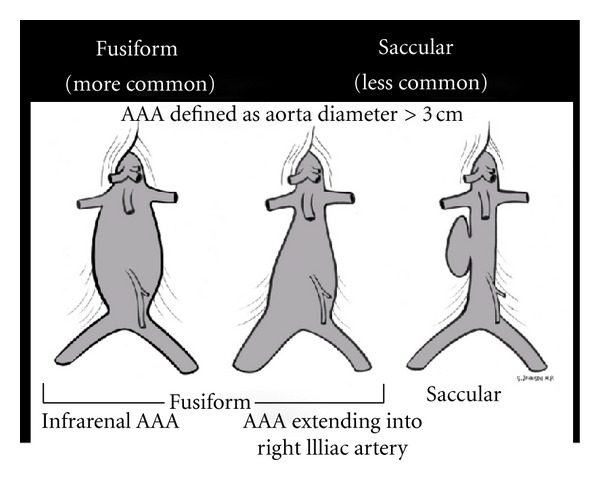
Abdominal aortic aneurysm (AAA) types.
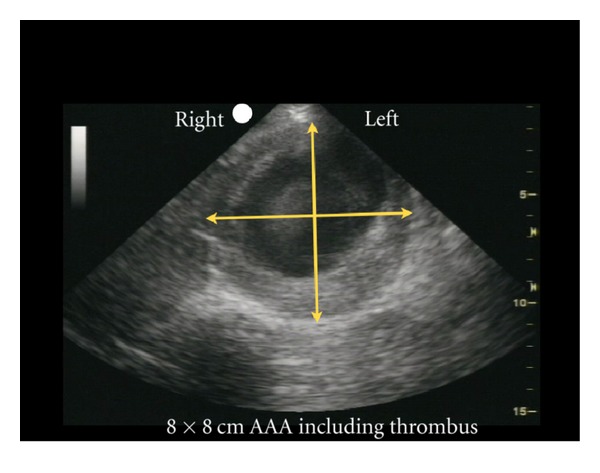
Abdominal aortic aneurysm (AAA) measured, short axis view.
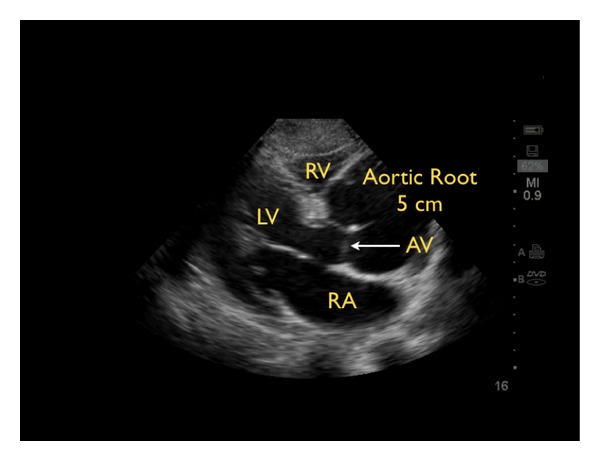
Aortic arch dissection with widened aortic root, parasternal long axis view. RV: right ventricle, LV: left ventricle, LA: left atrium, AV: aortic valve.
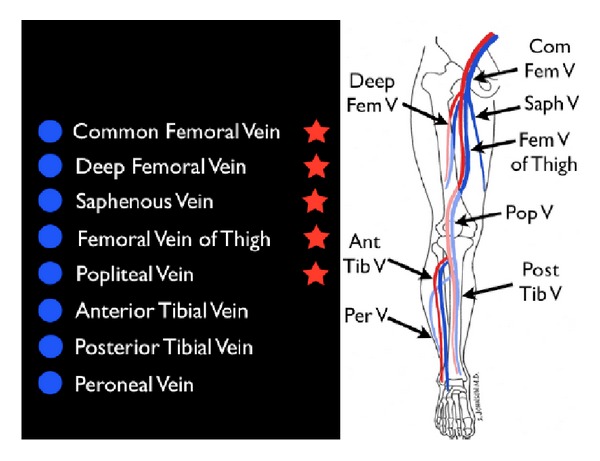
Limited leg deep venous thrombosis exam (starred veins).
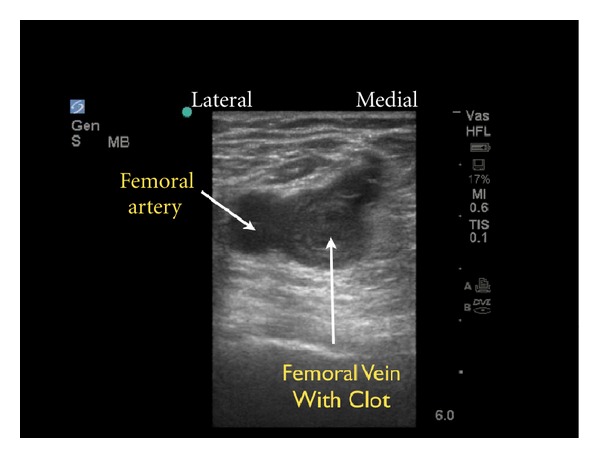
Deep venous thrombosis of the femoral vein, short axis view.
References
-
- Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. The New England Journal of Medicine. 2001;345(19):1368–1377. - PubMed
-
- Sebat F, Musthafa AA, Johnson D, et al. Effect of a rapid response system for patients in shock on time to treatment and mortality during 5 years. Critical Care Medicine. 2007;35(11):2568–2575. - PubMed
-
- Jones AE, Tayal VS, Sullivan DM, Kline JA. Randomized, controlled trial of immediate versus delayed goal-directed ultrasound to identify the cause of nontraumatic hypotension in emergency department patients. Critical Care Medicine. 2004;32(8):1703–1708. - PubMed
-
- Atkinson PRT, McAuley DJ, Kendall RJ, et al. Abdominal and Cardiac Evaluation with Sonography in Shock (ACES): an approach by emergency physicians for the use of ultrasound in patients with undifferentiated hypotension. Emergency Medicine Journal. 2009;26(2):87–91. - PubMed
-
- Gunst M, Ghaemmaghami V, Sperry J, et al. Accuracy of cardiac function and volume status estimates using the bedside echocardiographic assessment in trauma/critical care. The Journal of Trauma. 2008;65(3):509–516. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Research Materials
