

Increased fetal insulin concentrations for one week fail to improve insulin secretion or β-cell mass in fetal sheep with chronically reduced glucose supply
- PMID: 23135788
- PMCID: PMC3543651
- DOI: 10.1152/ajpregu.00413.2012
Increased fetal insulin concentrations for one week fail to improve insulin secretion or β-cell mass in fetal sheep with chronically reduced glucose supply
Abstract
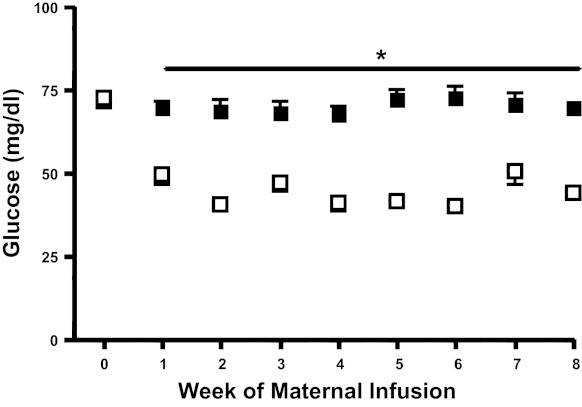
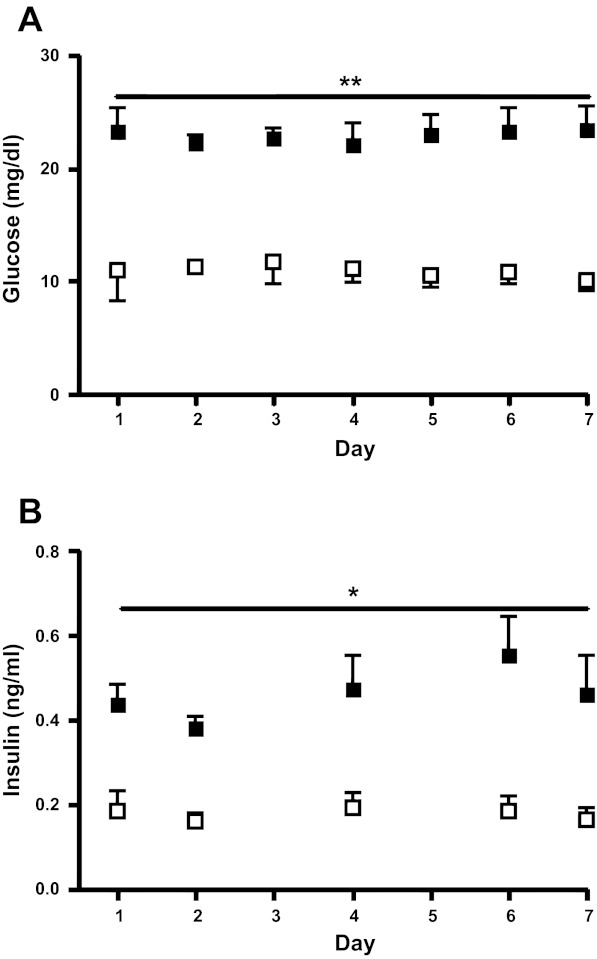
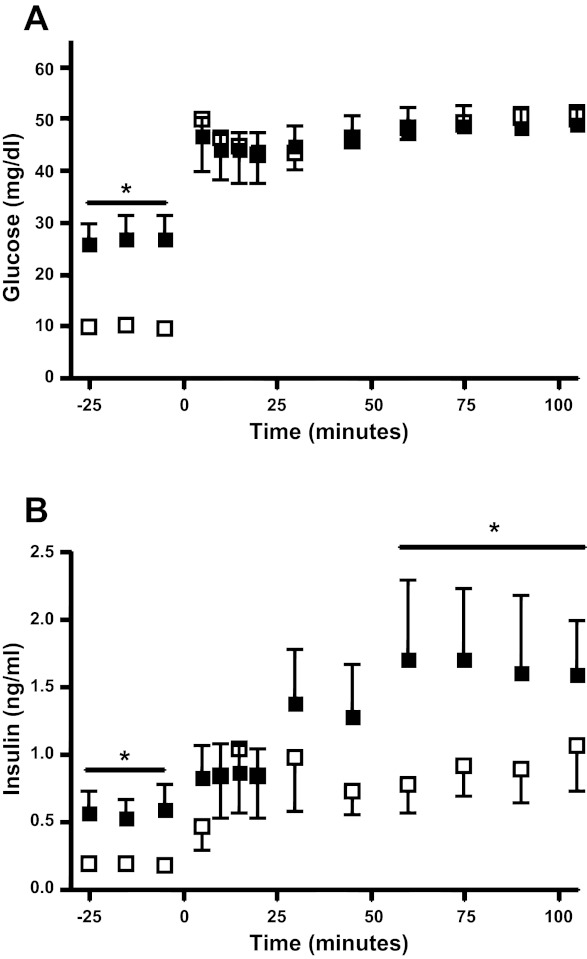
Maternal undernutrition during pregnancy and placental insufficiency are characterized by impaired development of fetal pancreatic β-cells. Prolonged reduced glucose supply to the fetus is a feature of both. It is unknown if reduced glucose supply, independent of other complications of maternal undernutrition and placental insufficiency, would cause similar β-cell defects. Therefore, we measured fetal insulin secretion and β-cell mass following prolonged reduced fetal glucose supply in sheep. We also tested whether restoring physiological insulin concentrations would correct any β-cell defects. Pregnant sheep received either a direct saline infusion (CON = control, n = 5) or an insulin infusion (HG = hypoglycemic, n = 5) for 8 wk in late gestation (75 to 134 days) to decrease maternal glucose concentrations and reduce fetal glucose supply. A separate group of HG fetuses also received a direct fetal insulin infusion for the final week of the study with a dextrose infusion to prevent a further fall in glucose concentration [hypoglycemic + insulin (HG+I), n = 4]. Maximum glucose-stimulated insulin concentrations were 45% lower in HG fetuses compared with CON fetuses. β-Cell, pancreatic, and fetal mass were 50%, 37%, and 40% lower in HG compared with CON fetuses, respectively (P < 0.05). Insulin secretion and β-cell mass did not improve in the HG+I fetuses. These results indicate that chronically reduced fetal glucose supply is sufficient to reduce pancreatic insulin secretion in response to glucose, primarily due to reduced pancreatic and β-cell mass, and is not correctable with insulin.
Figures
References
-
- Abayomi JC, Watkinson H, Boothby J, Topping J, Hackett AF. Identification of “hot spots” of obesity and being underweight in early pregnancy in Liverpool. J Hum Nutr Diet 22: 246–254, 2009 - PubMed
-
- Aspinwall CA, Lakey JR, Kennedy RT. Insulin-stimulated insulin secretion in single pancreatic beta cells. J Biol Chem 274: 6360–6365, 1999 - PubMed
-
- Belkacemi L, Nelson DM, Desai M, Ross MG. Maternal undernutrition influences placental-fetal development. Biol Reprod 83: 325–331, 2010 - PubMed
-
- Bloomfield FH. How is maternal nutrition related to preterm birth? Annu Rev Nutr 31: 235–261, 2011 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical