

Impact of strain typing methods on assessment of relationship between paired nares and wound isolates of methicillin-resistant Staphylococcus aureus
- PMID: 23135945
- PMCID: PMC3536221
- DOI: 10.1128/JCM.02423-12
Impact of strain typing methods on assessment of relationship between paired nares and wound isolates of methicillin-resistant Staphylococcus aureus
Abstract
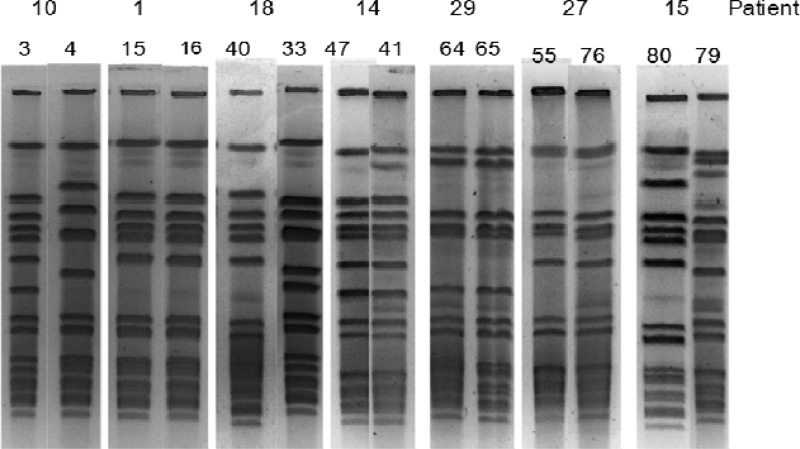
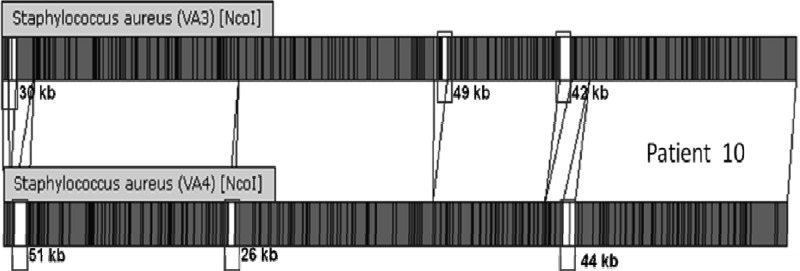
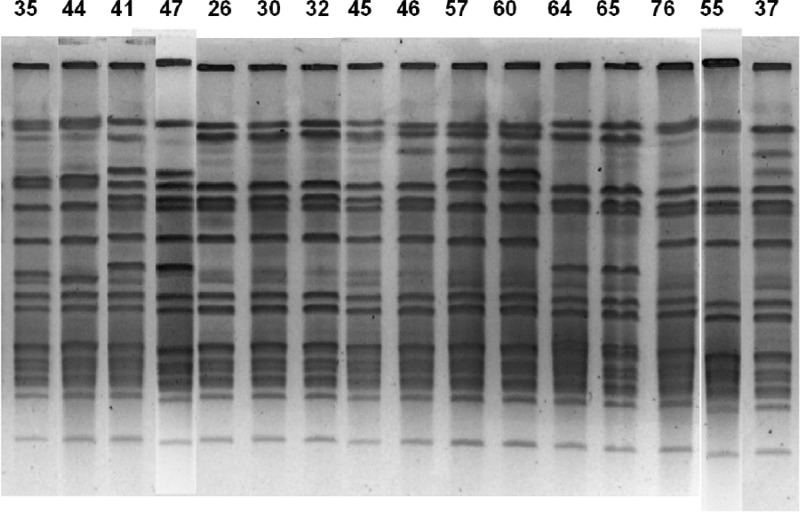
The anterior nares are the site of choice for the Veterans Administration methicillin-resistant Staphylococcus aureus (MRSA) surveillance program; however, a correlation between nares colonization and concomitant wound infections has not been well established. The purpose of this study was 3-fold: to determine the relatedness of MRSA isolates from 40 paired wound and nares specimens by four different strain typing methods, to determine concordance of typing methods, and to establish a baseline of MRSA types at this medical center. Isolates were typed by repetitive PCR (rep-PCR) (DiversiLab System; DL) and SpectraCell Raman analysis (SCRA) (commercially available methods that can be performed within a clinical lab), pulsed-field gel electrophoresis (PFGE), and an antibiotic susceptibility profile (AB). Whole-genome optical mapping (WGM) (OpGen, Inc.) was performed on selected isolates. All methods agreed that 26 pairs were indistinguishable and four pairs were different. Discrepant results were as follows: 4 where only SCRA was discordant, 3 where only AB was discordant, 2 where both DL and AB were discordant, and 1 where both DL and SCRA were discordant. All WGM agreed with PFGE. After discrepancy resolution, 80% of the pairs were indistinguishable and 20% were different. A total of 56% of nares results were nonpredictive if negative nares and positive wound cultures are included. Methods agreed 85 to 93% of the time; however, congruence of isolates to a clade was lower. Baseline analysis of types showed that 15 pairs were unique to single patients (30 strains, 38%; 47% of the matching pairs). Twenty-five strains (30%) represented a single clade identical by PFGE, SCRA, and DL, decreasing specificity. Typing method and institutional type frequency are important in assessing MRSA strain relatedness.
Figures
References
-
- Caffrey AR, Laplante KL. 2012. Changing epidemiology of methicillin-resistant Staphylococcus aureus in the Veterans Affairs Healthcare System, 2002-2009. Infection 40:291–297 - PubMed
-
- Jain R, Kralovic SM, Evans ME, Ambrose M, Simbartl LA, Obrosky DS, Render ML, Freyberg RW, Jernigan JA, Muder RR, Miller LJ, Roselle GA. 2011. Veterans Affairs initiative to prevent methicillin-resistant Staphylococcus aureus infections. N. Engl. J. Med. 364:1419–1430 - PubMed
-
- von Eiff C, Becker K, Machka K, Stammer H, Peters G. 2001. Nasal carriage as a source of Staphylococcus aureus bacteremia. N. Engl. J. Med. 344:11–16 - PubMed
-
- van Belkum A. 2007. Tracing isolates of bacterial species by multilocus variable number of tandem repeat analysis (MLVA). FEMS Immunol. Med. Microbiol. 49:22–27 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
