

Etiology of insulin resistance in youth with type 2 diabetes
- PMID: 23135953
- PMCID: PMC4296020
- DOI: 10.1007/s11892-012-0341-0
Etiology of insulin resistance in youth with type 2 diabetes
Abstract
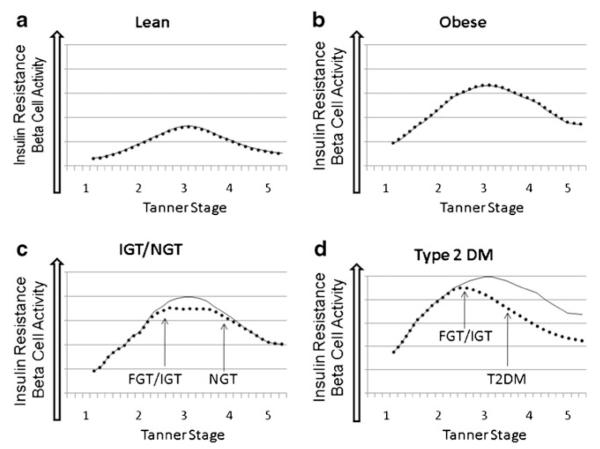
Type 2 diabetes (T2DM), historically an adult disease, is now increasingly prevalent in obese youth. Poor diet and increased sedentary behavior contribute to the increasing rates of obesity in youth, yet not all obese children develop T2DM. In general, T2DM is characterized by both insulin resistance (IR) and pancreatic beta-cell insufficiency. In children, IR is related to elevated body mass index (BMI) and pubertal hormones, along with abnormal fat partitioning, elevated free fatty acids, inflammation, and/or mitochondrial dysfunction. Hyperglycemia and T2DM develop when the pancreas cannot match the increased insulin demands resulting from IR. Unique to youth, IR varies with stage of pubertal development, and some children may have resolution of hyperglycemia post-puberty once the IR of puberty resolves. Further understanding of IR, the progression to T2DM in youth, and later outcomes as adults will help direct future therapies and interventions for youth at risk.
Figures
References
-
- Arslanian S, Suprasongsin C. Insulin sensitivity, lipids, and body composition in childhood: is “syndrome X” present? J Clin Endocrinol Metab. 1996;81(3):1058–62. - PubMed
-
- Ogden C, Carroll M, Kit B, Flegal K. Prevalence of obesity in the United States, 2009–2010 NCHS data brief, no 82. National Center for Health Statistics; Hyattsville. MD: 2012.
-
- Lee S, Bacha F, Gungor N, Arslanian S. Comparison of different definitions of pediatric metabolic syndrome: relation to abdominal adiposity, insulin resistance, adiponectin, and inflammatory biomarkers. J Pediatr. 2008;152(2):177–84. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
