

Defining falciparum-malaria-attributable severe febrile illness in moderate-to-high transmission settings on the basis of plasma PfHRP2 concentration
- PMID: 23136222
- PMCID: PMC3532834
- DOI: 10.1093/infdis/jis675
Defining falciparum-malaria-attributable severe febrile illness in moderate-to-high transmission settings on the basis of plasma PfHRP2 concentration
Abstract
Background: In malaria-endemic settings, asymptomatic parasitemia complicates the diagnosis of malaria. Histidine-rich protein 2 (HRP2) is produced by Plasmodium falciparum, and its plasma concentration reflects the total body parasite burden. We aimed to define the malaria-attributable fraction of severe febrile illness, using the distributions of plasma P. falciparum HRP2 (PfHRP2) concentrations from parasitemic children with different clinical presentations.
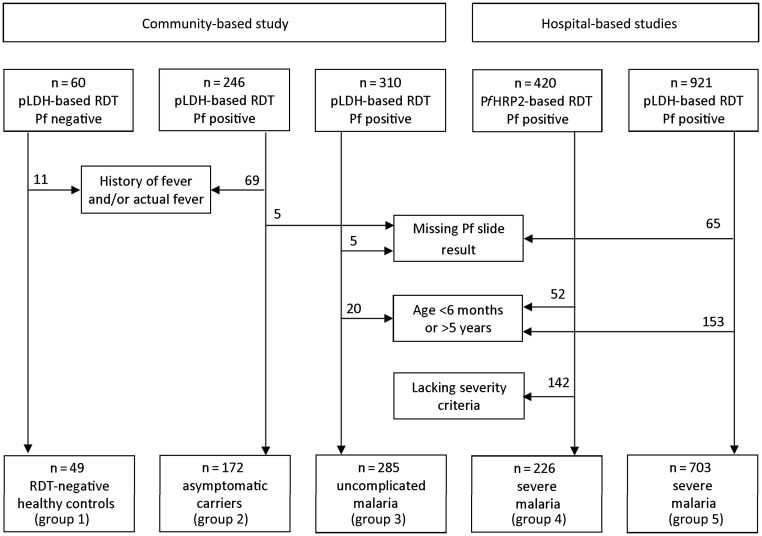
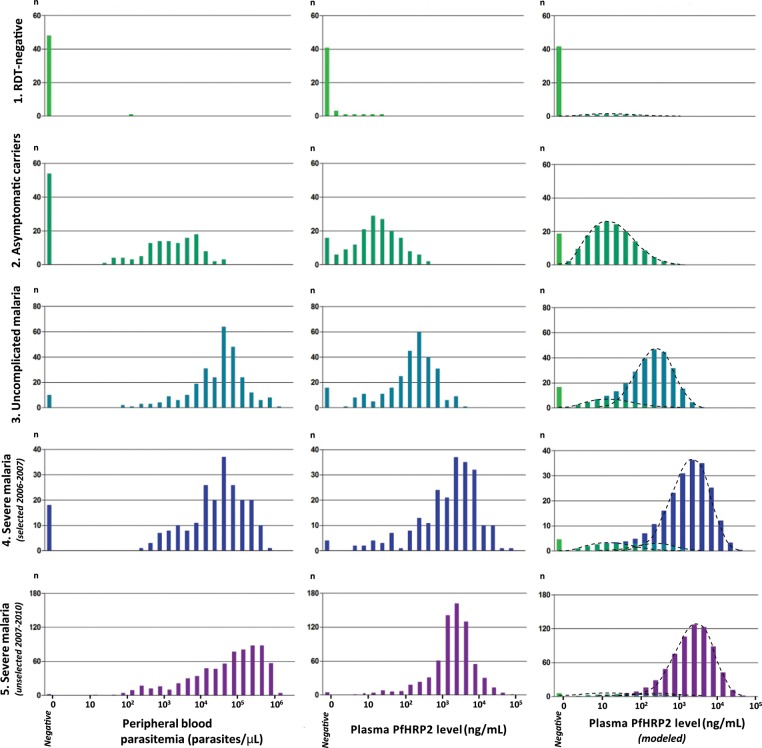
Methods: Plasma samples were collected from and peripheral blood slides prepared for 1435 children aged 6-60 months in communities and a nearby hospital in northeastern Tanzania. The study population included children with severe or uncomplicated malaria, asymptomatic carriers, and healthy control subjects who had negative results of rapid diagnostic tests. The distributions of plasma PfHRP2 concentrations among the different groups were used to model severe malaria-attributable disease.
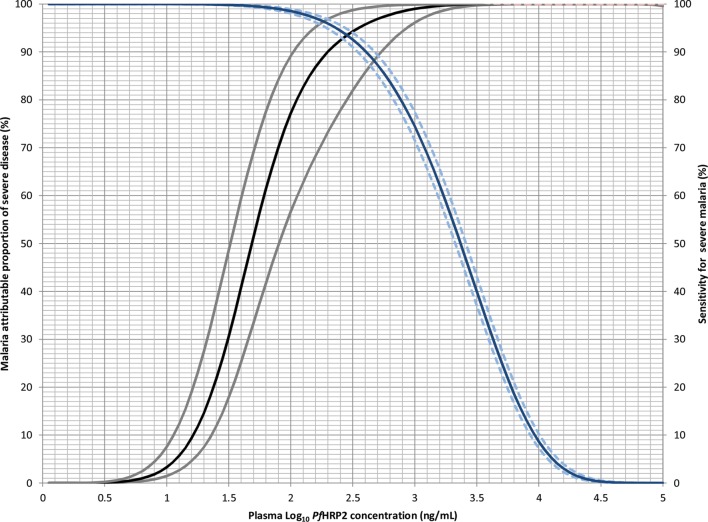
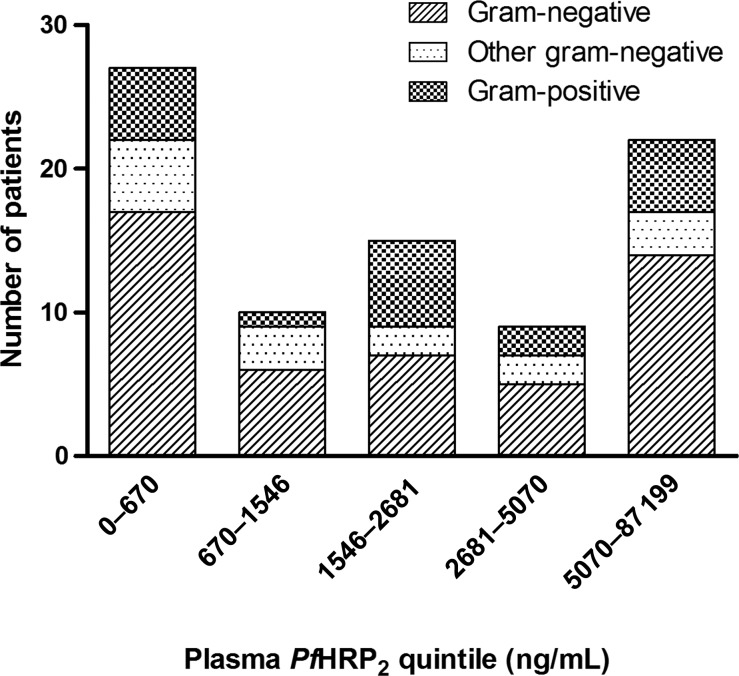
Results: The plasma PfHRP2 concentration showed a close correlation with the severity of infection. PfHRP2 concentrations of >1000 ng/mL denoted a malaria-attributable fraction of severe disease of 99% (95% credible interval [CI], 96%-100%), with a sensitivity of 74% (95% CI, 72%-77%), whereas a concentration of <200 ng/mL denoted severe febrile illness of an alternative diagnosis in >10% (95% CI, 3%-27%) of patients. Bacteremia was more common among patients in the lowest and highest PfHRP2 concentration quintiles.
Conclusions: The plasma PfHRP2 concentration defines malaria-attributable disease and distinguishes severe malaria from coincidental parasitemia in African children in a moderate-to-high transmission setting.
Figures
References
-
- Black RE, Cousens S, Johnson HL, et al. Global, regional, and national causes of child mortality in 2008: a systematic analysis. Lancet. 2010;375:1969–87. - PubMed
-
- Abdullah S, Adazu K, Masanja H, et al. Patterns of age-specific mortality in children in endemic areas of sub-Saharan Africa. Am J Trop Med Hyg. 2007;77:99–105. - PubMed
-
- Murray CJ, Rosenfeld LC, Lim SS, et al. Global malaria mortality between 1980 and 2010: a systematic analysis. Lancet. 2012;379:413–31. - PubMed
-
- Snow RW, Nahlen B, Palmer A, Donnelly CA, Gupta S, Marsh K. Risk of severe malaria among African infants: direct evidence of clinical protection during early infancy. J Infect Dis. 1998;177:819–22. - PubMed
