

From randomized trials to the clinic: is it time to implement individual lung-cancer screening in clinical practice? A multidisciplinary statement from French experts on behalf of the French intergroup (IFCT) and the groupe d'Oncologie de langue francaise (GOLF)
- PMID: 23136229
- PMCID: PMC3574545
- DOI: 10.1093/annonc/mds476
From randomized trials to the clinic: is it time to implement individual lung-cancer screening in clinical practice? A multidisciplinary statement from French experts on behalf of the French intergroup (IFCT) and the groupe d'Oncologie de langue francaise (GOLF)
Abstract
Background: Despite advances in cancer therapy, mortality is still high except in early-stage tumors, and screening remains a challenge. The randomized National Lung Screening Trial (NLST), comparing annual low-dose computed tomography (LDCT) and chest X-rays, revealed a 20% decrease in lung-cancer-specific mortality. These results raised numerous questions. The French intergroup for thoracic oncology and the French-speaking oncology group convened an expert group to provide a coherent outlook on screening modalities in France.
Methods: A literature review was carried out and transmitted to the expert group, which was divided into three workshops to tackle specific questions, with responses presented in a plenary session. A writing committee drafted this article.
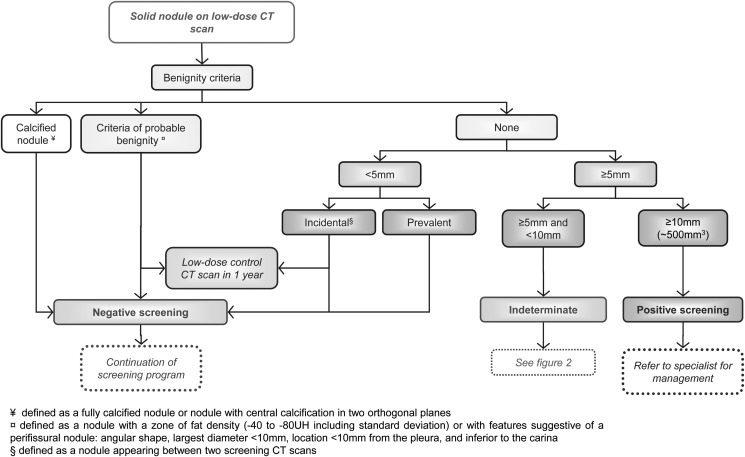
Results: The multidisciplinary group favored individual screening in France, when carried out as outlined in this article and after informing subjects of the benefits and risks. The target population involves subjects aged 55-74 years, who are smokers or have a 30 pack-year smoking history. Subjects should be informed about the benefits of quitting. Screening should involve LDCT scanning with specific modalities. Criteria for CT positivity and management algorithms for positive examinations are given.
Conclusions: Individual screening requires rigorous assessment and precise research in order to potentially develop a lung-cancer screening policy.
Figures


Similar articles
-
Baseline results of the Depiscan study: a French randomized pilot trial of lung cancer screening comparing low dose CT scan (LDCT) and chest X-ray (CXR).Lung Cancer. 2007 Oct;58(1):50-8. doi: 10.1016/j.lungcan.2007.05.009. Epub 2007 Jul 12. Lung Cancer. 2007. PMID: 17624475 Clinical Trial.
-
Long-Term Follow-up Results of the DANTE Trial, a Randomized Study of Lung Cancer Screening with Spiral Computed Tomography.Am J Respir Crit Care Med. 2015 May 15;191(10):1166-75. doi: 10.1164/rccm.201408-1475OC. Am J Respir Crit Care Med. 2015. PMID: 25760561 Clinical Trial.
-
[China National Lung Cancer Screening Guideline with Low-dose Computed Tomography (2018 version)].Zhongguo Fei Ai Za Zhi. 2018 Feb 20;21(2):67-75. doi: 10.3779/j.issn.1009-3419.2018.02.01. Zhongguo Fei Ai Za Zhi. 2018. PMID: 29526173 Free PMC article. Chinese.
-
Screening for Lung Cancer With Low-Dose Computed Tomography: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force.JAMA. 2021 Mar 9;325(10):971-987. doi: 10.1001/jama.2021.0377. JAMA. 2021. PMID: 33687468
-
Screening for lung cancer: time for large-scale screening by chest computed tomography.Eur Respir J. 2014 Jul;44(1):217-38. doi: 10.1183/09031936.00164513. Epub 2014 Feb 13. Eur Respir J. 2014. PMID: 24525442 Review.
Cited by
-
Multi-Biomarkers Panel in Identifying Benign and Malignant Lung Diseases and Pathological Types of Lung Cancer.J Cancer. 2023 Jun 26;14(10):1904-1912. doi: 10.7150/jca.85846. eCollection 2023. J Cancer. 2023. PMID: 37476198 Free PMC article.
-
Evaluation of the lung cancer risks at which to screen ever- and never-smokers: screening rules applied to the PLCO and NLST cohorts.PLoS Med. 2014 Dec 2;11(12):e1001764. doi: 10.1371/journal.pmed.1001764. eCollection 2014 Dec. PLoS Med. 2014. PMID: 25460915 Free PMC article.
-
Lung Cancer Screening Using Low Dose CT Scanning in Germany. Extrapolation of results from the National Lung Screening Trial.Dtsch Arztebl Int. 2015 Sep 18;112(38):637-44. doi: 10.3238/arztebl.2015.0637. Dtsch Arztebl Int. 2015. PMID: 26429636 Free PMC article. Clinical Trial.
-
Medical follow-up of workers exposed to lung carcinogens: French evidence-based and pragmatic recommendations.BMC Public Health. 2017 Feb 14;17(1):191. doi: 10.1186/s12889-017-4114-1. BMC Public Health. 2017. PMID: 28193266 Free PMC article.
-
Annual or biennial lung cancer CT screening?J Thorac Dis. 2016 Sep;8(9):2424-2426. doi: 10.21037/jtd.2016.09.20. J Thorac Dis. 2016. PMID: 27746993 Free PMC article. No abstract available.
References
-
- Henschke CI, Yankelevitz DF, Libby DM, et al. Survival of patients with stage I lung cancer detected on CT screening. N Engl J Med. 2006;355(17):1763–1771. - PubMed
-
- Raz DJ, Zell JA, Ou S-HI, et al. Natural History of Stage I Non-Small Cell Lung Cancer: Implications for Early Detection. Chest. 2007;132(1):193–199. - PubMed
-
- Nawa T, Nakagawa T, Mizoue T, et al. Long-term prognosis of patients with lung cancer detected on low-dose chest computed tomography screening. Lung Cancer. 2012;75(2):197–202. - PubMed
-
- Frost JK, Ball WC, Jr, Levin ML, et al. Early lung cancer detection: results of the initial (prevalence) radiologic and cytologic screening in the Johns Hopkins study. Am Rev Respir Dis. 1984;130(4):549–554. - PubMed
-
- Marcus PM, Bergstralh EJ, Fagerstrom RM, et al. Lung cancer mortality in the Mayo Lung Project: impact of extended follow-up. J Natl Cancer Inst. 2000;92(16):1308–1316. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
