

Atypical manifestations and poor outcome of herpes simplex encephalitis in the immunocompromised
- PMID: 23136265
- PMCID: PMC3511927
- DOI: 10.1212/WNL.0b013e3182752ceb
Atypical manifestations and poor outcome of herpes simplex encephalitis in the immunocompromised
Abstract
Objective: To characterize clinical features, neuroimaging, and outcomes of herpes simplex encephalitis (HSE) in immunocompromised individuals.
Methods: We performed a retrospective case control review of patients diagnosed with HSE. Adult patients were dichotomized into immunocompromised (n = 14) and immunocompetent groups (n = 15).
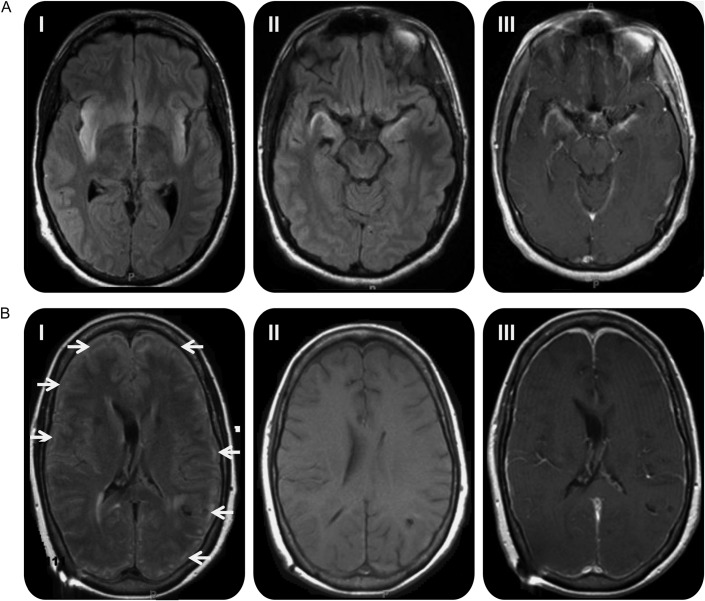
Results: Fewer immunocompromised patients presented with prodromal symptoms and focal deficits. While the majority of CSF profiles in the immunocompromised patients were mononuclear cells predominant, 3 had polymorphonuclear predominance and another 3 had normal profiles. MRI showed widespread cortical involvement, with brainstem or cerebellar involvement in some. Two immunocompromised patients had recurrent HSE. The immunosuppressed state was associated with a decrease in Karnofsky Performance Status Scale (KPSS) score of 23.1 (p = 0.018). Every 1-day delay in initiation of acyclovir was associated with a decrease in KPSS of 10.2 (p = 0.002), and every 10 cell/mm(3) increase of CSF leukocytosis was associated with an increase in KPSS of 0.7 (p = 0.009). Mortality rate was 6 times higher in the immunocompromised patients.
Conclusions: Immunocompromised states may predispose to HSE with atypical clinical and neuroradiologic features. Immunocompromised individuals with HSE have significantly worse outcomes and mortality. Early diagnosis and treatment is associated with improved outcome. The findings are particularly important in light of the increasing use of potent immunosuppressive and immunomodulatory therapies.
Figures
Comment in
-
Re: Atypical manifestations and poor outcome of herpes simplex encephalitis in the immunocompromised.Neurology. 2013 Jul 30;81(5):514. doi: 10.1212/01.wnl.0000433164.29848.92. Neurology. 2013. PMID: 23897880 No abstract available.
-
Author response.Neurology. 2013 Jul 30;81(5):514. Neurology. 2013. PMID: 24058941 No abstract available.
References
-
- Granerod J, Ambrose HE, Davies NW, et al. Causes of encephalitis and differences in their clinical presentations in England: a multicentre, population-based prospective study. Lancet Infect Dis 2010;10:835–844 - PubMed
-
- Hjalmarsson A, Blomqvist P, Skoldenberg B. Herpes simplex encephalitis in Sweden, 1990–2001: incidence, morbidity, and mortality. Clin Infect Dis 2007;45:875–880 - PubMed
-
- Whitley RJ. Herpes simplex encephalitis: adolescents and adults. Antiviral Res 2006;71:141–148 - PubMed
-
- Rozenberg F, Deback C, Agut H. Herpes simplex encephalitis: from virus to therapy. Infect Disord Drug Targets 2011;11:235–250 - PubMed
-
- Whitley RJ, Alford CA, Hirsch MS, et al. Vidarabine versus acyclovir therapy in herpes simplex encephalitis. N Engl J Med 1986;314:144–149 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources