

Impact of community management of fever (using antimalarials with or without antibiotics) on childhood mortality: a cluster-randomized controlled trial in Ghana
- PMID: 23136273
- PMCID: PMC3748510
- DOI: 10.4269/ajtmh.2012.12-0078
Impact of community management of fever (using antimalarials with or without antibiotics) on childhood mortality: a cluster-randomized controlled trial in Ghana
Abstract
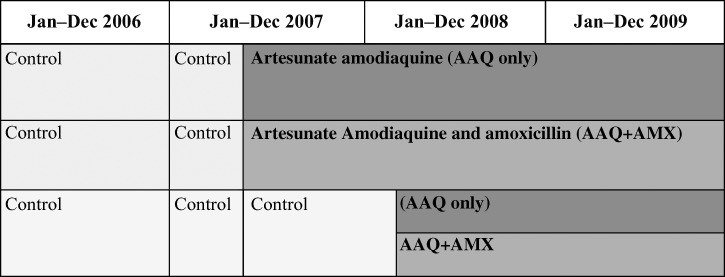
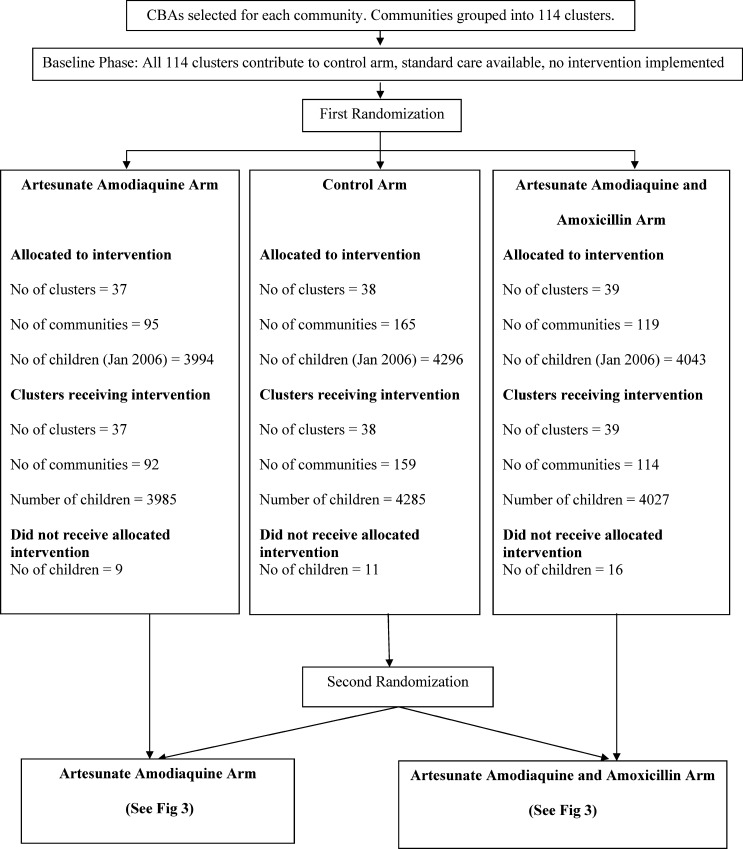
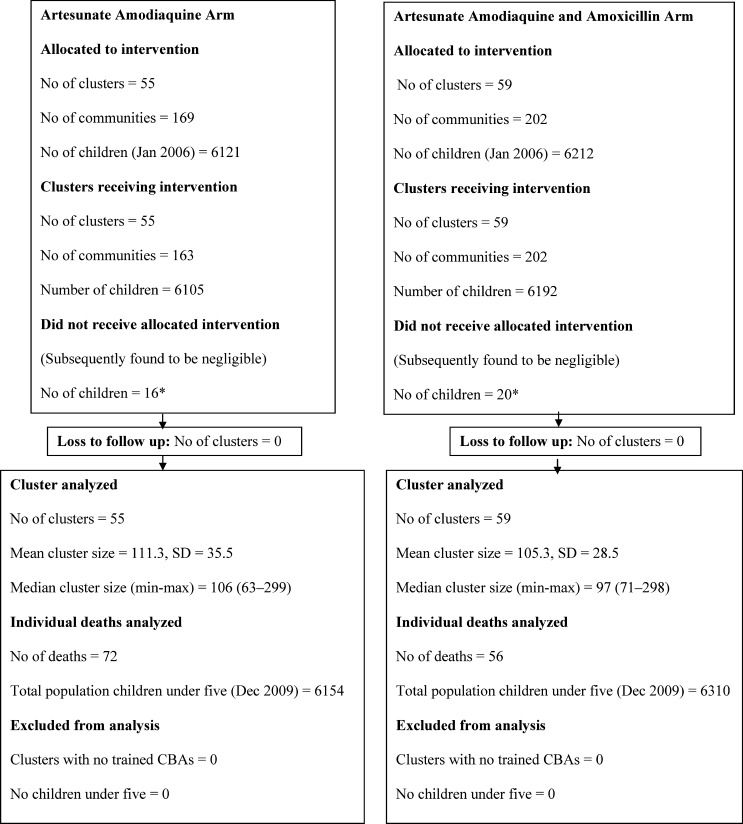
Malaria and pneumonia are leading causes of childhood mortality. Home Management of fever as Malaria (HMM) enables presumptive treatment with antimalarial drugs but excludes pneumonia. We aimed to evaluate the impact of adding an antibiotic, amoxicillin (AMX) to an antimalarial, artesunate amodiaquine (AAQ + AMX) for treating fever among children 2-59 months of age within the HMM strategy on all-cause mortality. In a stepped-wedge cluster-randomized, open trial, children 2-59 months of age with fever treated with AAQ or AAQ + AMX within HMM were compared with standard care. Mortality reduced significantly by 30% (rate ratio [RR] = 0.70, 95% confidence interval [CI] = 0.53-0.92, P = 0.011) in AAQ clusters and by 44% (RR = 0.56, 95% CI = 0.41-0.76, P = 0.011) in AAQ + AMX clusters compared with control clusters. The 21% mortality reduction between AAQ and AAQ + AMX (RR = 0.79, 95% CI = 0.56-1.12, P = 0.195) was however not statistically significant. Community fever management with antimalarials significantly reduces under-five mortality. Given the lower mortality trend, adding an antibiotic is more beneficial.
Conflict of interest statement
Disclosure: TDR/UNDP Trial registration. A: 20189: The trial protocol can be accessed from the WHO (Ethics Committee).
Figures
References
-
- Black RE, Morris SS, Bryce J. Where and why are 10 million children dying every year? Lancet. 2003;361:2226–2234. - PubMed
-
- UNICEF . Children and the Millennium Development Goals: Progress Towards a World Fit for Children. New York: United Nations Children's Fund; 2007.
-
- UNICEF . State of the World's Children, 2008. New York: United Nations Children's Fund; 2007.
-
- Schellenberg JA, Victora CG, Mushi A, de Savigny D, Schellenberg D, Mshinda H, Bryce J. For the Tanzania IMCI MCE baseline household survey study group. Inequalities among the very poor: health care for children in rural southern Tanzania. Lancet. 2003;361:561–566. - PubMed
-
- Family Health Division of the Ghana Health Service . Child Situation Analysis. Accra; Ghana: 2007.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
