

30-day in-hospital mortality after acute myocardial infarction in Tuscany (Italy): an observational study using hospital discharge data
- PMID: 23136904
- PMCID: PMC3507800
- DOI: 10.1186/1471-2288-12-170
30-day in-hospital mortality after acute myocardial infarction in Tuscany (Italy): an observational study using hospital discharge data
Abstract
Background: Coronary heart disease is the leading cause of mortality in the world. One of the outcome indicators recently used to measure hospital performance is 30-day mortality after acute myocardial infarction (AMI). This indicator has proven to be a valid and reproducible indicator of the appropriateness and effectiveness of the diagnostic and therapeutic process for AMI patients after hospital admission. The aim of this study was to examine the determinants of inter-hospital variability on 30-day in-hospital mortality after AMI in Tuscany. This indicator is a proxy of 30-day mortality that includes only deaths occurred during the index or subsequent hospitalizations.
Methods: The study population was identified from hospital discharge records (HDRs) and included all patients with primary or secondary ICD-9-CM codes of AMI (ICD-9 codes 410.xx) that were discharged between January 1, 2009 and November 30, 2009 from any hospital in Tuscany. The outcome of interest was 30-day all-cause in-hospital mortality, defined as a death occurring for any reason in the hospital within 30 days of the admission date. Because of the hierarchical structure of the data, with patients clustered into hospitals, random-effects (multilevel) logistic regression models were used. The models included patient risk factors and random intercepts for each hospital.
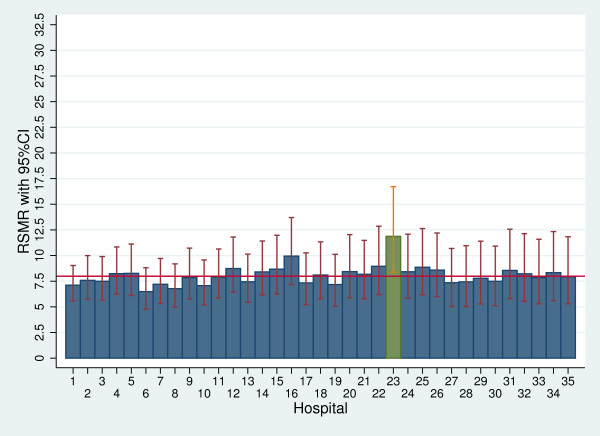
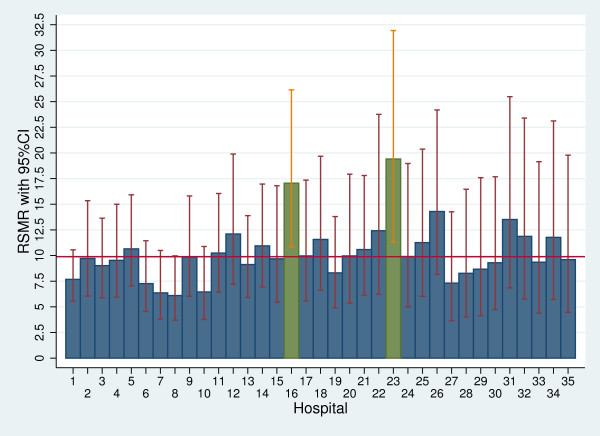
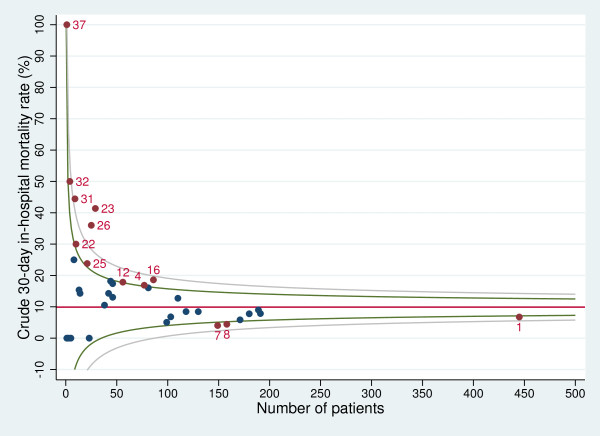
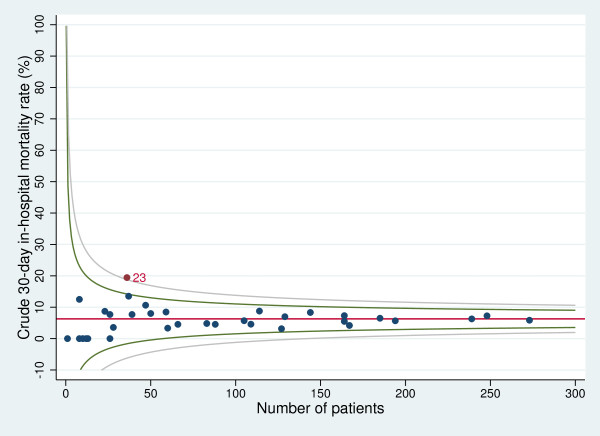
Results: The study included 5,832 patients, 61.90% male, with a mean age of 72.38 years. During the study period, 7.99% of patients died within 30 days of admission. The 30-day in-hospital mortality rate was significantly higher among patients with ST segment elevation myocardial infarction (STEMI) compared with those with non-ST segment elevation myocardial infarction (NSTEMI). The multilevel analysis which included only the hospital variance showed a significant inter-hospital variation in 30-day in-hospital mortality. When patient characteristics were added to the model, the hospital variance decreased. The multilevel analysis was then carried out separately in the two strata of patients with STEMI and NSTEMI. In the STEMI group, after adjusting for patient characteristics, some residual inter-hospital variation was found, and was related to the presence of a cardiac catheterisation laboratory.
Conclusion: We have shown that it is possible to use routinely collected administrative data to predict mortality risk and to highlight inter-hospital differences. The distinction between STEMI and NSTEMI proved to be useful to detect organisational characteristics, which affected only the STEMI subgroup.
Figures
Similar articles
-
[Trends in occurrence, treatment, and outcomes of acute myocardial infarction in Tuscany Region (Central Italy), 1997-2010].Epidemiol Prev. 2015;39(3):167-75. Epidemiol Prev. 2015. PMID: 26668916 Italian.
-
Recent Trends in Hospitalization for Acute Myocardial Infarction in Beijing: Increasing Overall Burden and a Transition From ST-Segment Elevation to Non-ST-Segment Elevation Myocardial Infarction in a Population-Based Study.Medicine (Baltimore). 2016 Feb;95(5):e2677. doi: 10.1097/MD.0000000000002677. Medicine (Baltimore). 2016. PMID: 26844503 Free PMC article.
-
Epidemiology of acute myocardial infarction in the Italian CCU network: the BLITZ study.Eur Heart J. 2003 Sep;24(18):1616-29. doi: 10.1016/s0195-668x(03)00278-1. Eur Heart J. 2003. PMID: 14499224
-
COVID-19 Positive Status is Associated with Increased In-hospital Mortality in Patients with Acute Myocardial Infarction: A Systematic Review and Meta-analysis.J Community Hosp Intern Med Perspect. 2022 Sep 9;12(4):17-24. doi: 10.55729/2000-9666.1103. eCollection 2022. J Community Hosp Intern Med Perspect. 2022. PMID: 36348971 Free PMC article. Review.
-
Leveraging Clinical Digitized Data to Understand Temporal Characteristics and Outcomes of Acute Myocardial Infarctions at a Tertiary Care Medical Centre in Pakistan from 1988-2018 - Methods and Results.Glob Heart. 2022 Aug 18;17(1):58. doi: 10.5334/gh.1147. eCollection 2022. Glob Heart. 2022. PMID: 36051315 Free PMC article. Review.
Cited by
-
Differences in acute ischaemic stroke in-hospital mortality across referral stroke hospitals in Spain: a retrospective, longitudinal observational study.BMJ Open. 2023 Jun 28;13(6):e068183. doi: 10.1136/bmjopen-2022-068183. BMJ Open. 2023. PMID: 37380213 Free PMC article.
-
Electrocardiographic Predictors of Primary Ventricular Fibrillation and 30-Day Mortality in Patients Presenting with ST-Segment Elevation Myocardial Infarction.J Clin Med. 2021 Dec 17;10(24):5933. doi: 10.3390/jcm10245933. J Clin Med. 2021. PMID: 34945229 Free PMC article.
-
Glycoprotein IIb/IIIa inhibitors use and outcome after percutaneous coronary intervention for non-ST elevation myocardial infarction.Biomed Res Int. 2014;2014:643981. doi: 10.1155/2014/643981. Epub 2014 May 8. Biomed Res Int. 2014. PMID: 24895595 Free PMC article.
-
Educational level and 30-day outcomes after hospitalization for acute myocardial infarction in Italy.BMC Health Serv Res. 2017 Jan 9;17(1):18. doi: 10.1186/s12913-016-1966-5. BMC Health Serv Res. 2017. PMID: 28069004 Free PMC article.
-
Sudden cardiac death early after ST elevation myocardial infarction with and without severe left ventricular dysfunction.Indian Heart J. 2014 Nov-Dec;66(6):569-73. doi: 10.1016/j.ihj.2014.10.416. Epub 2014 Nov 14. Indian Heart J. 2014. PMID: 25634386 Free PMC article.
References
-
- Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ. Global Burden of Disease and Risk Factors. Oxford University press and The World Bank, New York; 2006. - PubMed
-
- Gale CP, Cattle BA, Woolston A, Baxter PD, West TH, Simms AD, Blaxill J, Greenwood DC, Fox KA, West RM. Resolving inequalities in care? Reduced mortality in the elderly after acute coronary syndromes. The Myocardial Ischaemia National Audit Project 2003–2010. Eur Heart J. 2012;33(5):630–639. doi: 10.1093/eurheartj/ehr381. - DOI - PubMed
-
- Chan MY, Sun JL, Newby LK, Shaw LK, Lin M, Peterson ED, Califf RM, Kong DF, Roe MT. Long-term mortality of patients undergoing cardiac catheterization for ST-elevation and non-ST-elevation myocardial infarction. Circulation. 2009;119(24):3110–3117. doi: 10.1161/CIRCULATIONAHA.108.799981. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
