

Impact of adjusting for the reciprocal relationship between maternal weight and free thyroxine during early pregnancy
- PMID: 23136959
- PMCID: PMC3569945
- DOI: 10.1089/thy.2012.0440
Impact of adjusting for the reciprocal relationship between maternal weight and free thyroxine during early pregnancy
Abstract
Background: Among euthyroid pregnant women in a large clinical trial, free thyroxine (FT4) measurements below the 2.5th centile were associated with a 17 lb higher weight (2.9 kg/m(2)) than in the overall study population. We explore this relationship further.
Methods: Among 9351 women with second trimester thyrotropin (TSH) measurements between 1st and 98th centiles, we examine: (i) the weight/FT4 relationship; (ii) percentages of women in three weight categories at each FT4 decile; (iii) FT4 concentrations in three weight categories at each TSH decile; and (iv) impact of adjusting FT4 for weight--in the reference group and in 190 additional women with elevated TSH measurements.
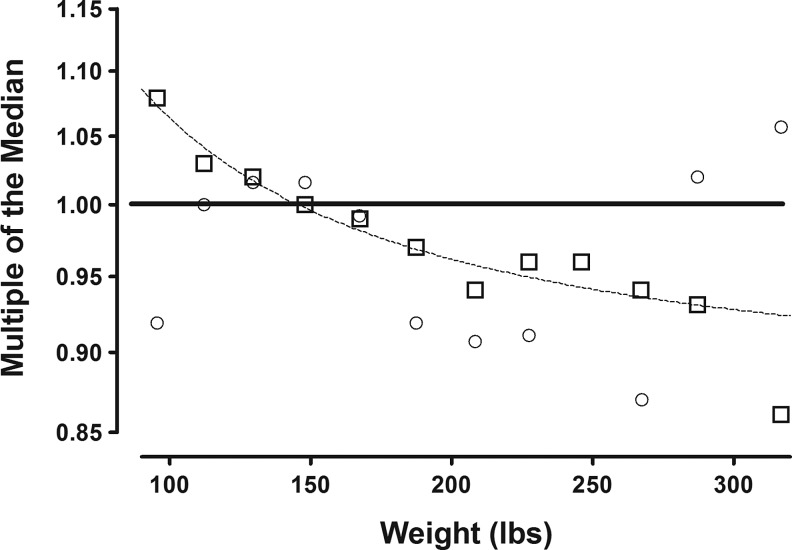
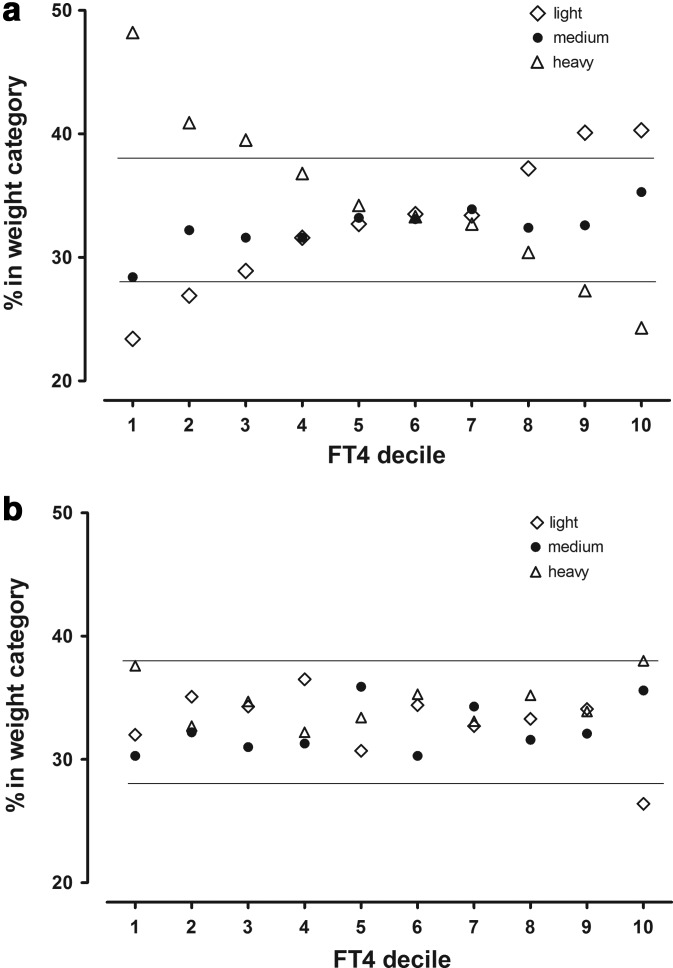
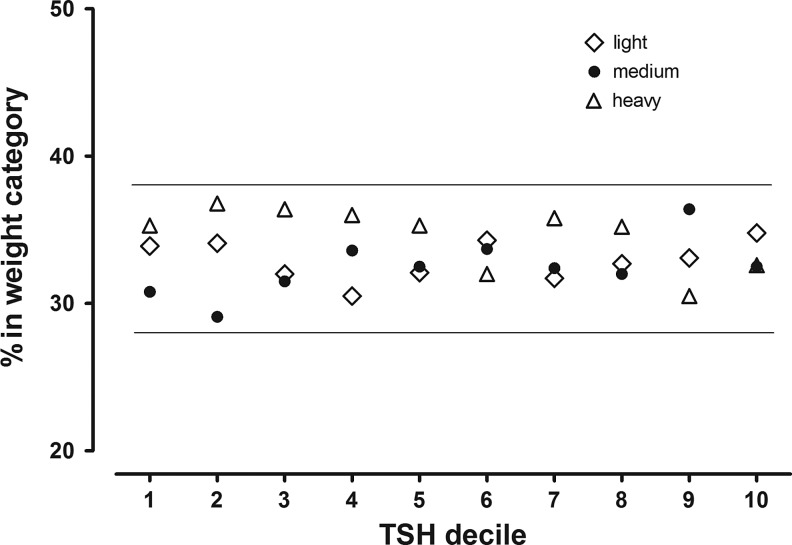
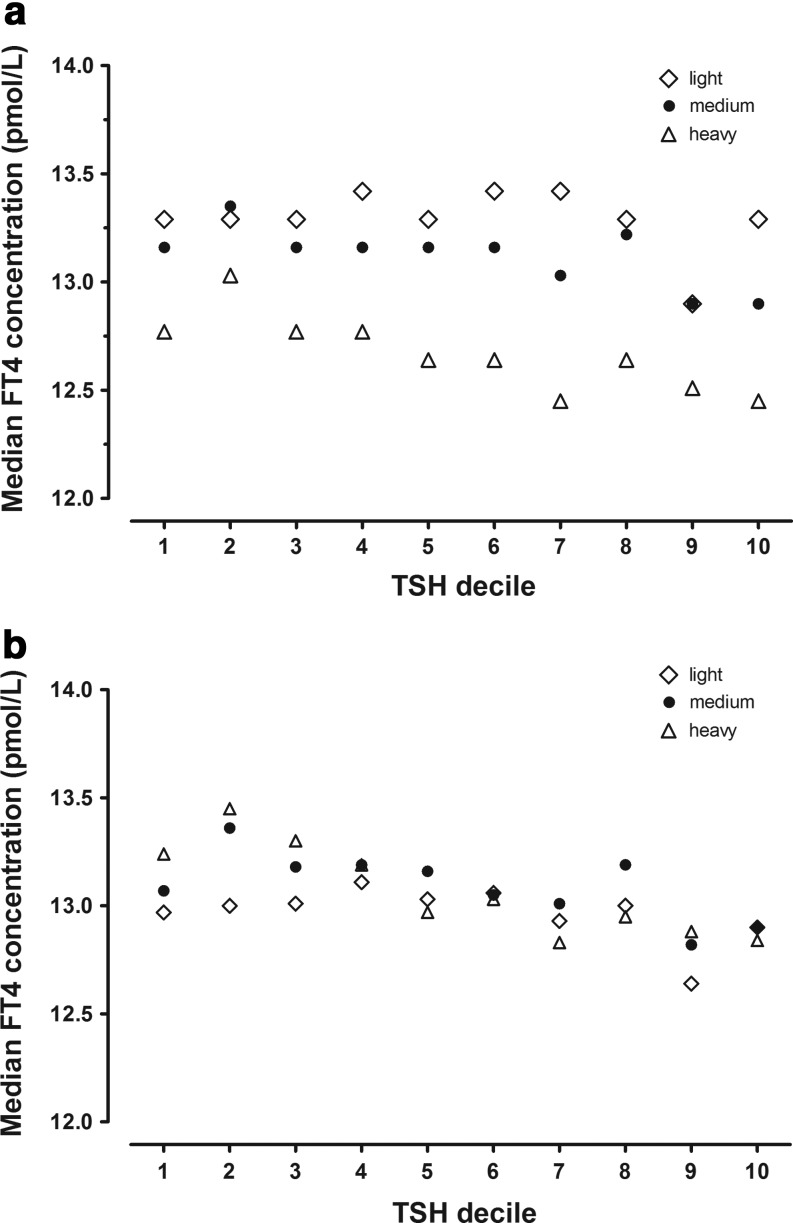
Results: FT4 values decrease steadily as weight increases (p<0.0001 by ANOVA) among women in the reference group (TSH 0.05-3.8 IU/L). TSH follows no consistent pattern with weight. When stratified into weight tertiles, 48% of women at the lowest FT4 decile are heavy; the percentage decreases steadily to 22% at the highest FT4 decile. Median FT4 is lowest in heaviest women regardless of the TSH level. In the reference group, weight adjustment reduces overall variance by 2.9%. Fewer FT4 measurements are at either extreme (below the 5th FT4 centile: 4.8% before adjustment, 4.7% after adjustment; above the 95th FT4 centile: 5.0% and 4.7%, respectively). Adjustment places more light weight women and fewer heavy women below the 5th FT4 centile; the converse above the 95th centile. Between TSH 3.8 and 5 IU/L, the FT4 percentage below the 5th FT4 centile is not elevated (3.8% before adjustment, 3.1% after adjustment). Percentage of FT4 values above the 95th centile, however, is lower (1.5% before adjustment, 0.8% after adjustment). Above TSH 5 IU/L, 25% of women have FT4 values below the 5th FT4 centile; weight adjustment raises this to 30%; no FT4 values remain above the 95th FT4 centile.
Conclusions: During early pregnancy, TSH values are not associated with weight, unlike nonpregnant adults. Lower average FT4 values among heavy women at all TSH deciles partially explain interindividual differences in FT4 reference ranges. The continuous reciprocal relationship between weight and FT4 explains lower FT4 with higher weight. Weight adjustment refines FT4 interpretation.
Figures
Similar articles
-
Trimester-specific thyroid hormone reference ranges in Sudanese women.BMC Physiol. 2016 Oct 31;16(1):5. doi: 10.1186/s12899-016-0025-0. BMC Physiol. 2016. PMID: 27795209 Free PMC article.
-
First- and second-trimester thyroid hormone reference data in pregnant women: a FaSTER (First- and Second-Trimester Evaluation of Risk for aneuploidy) Research Consortium study.Am J Obstet Gynecol. 2008 Jul;199(1):62.e1-6. doi: 10.1016/j.ajog.2007.12.003. Am J Obstet Gynecol. 2008. PMID: 18585522 Free PMC article.
-
Thyroid Function Reference Values in Healthy Iodine-Sufficient Pregnant Women and Influence of Thyroid Nodules on Thyrotropin and Free Thyroxine Values.Thyroid. 2019 Mar;29(3):421-429. doi: 10.1089/thy.2018.0324. Epub 2019 Feb 22. Thyroid. 2019. PMID: 30693851
-
Method-dependent variation in TSH and FT4 reference intervals in pregnancy: A systematic review.Ann Clin Biochem. 2021 Sep;58(5):537-546. doi: 10.1177/00045632211026955. Epub 2021 Jun 25. Ann Clin Biochem. 2021. PMID: 34120478
-
Childhood Thyroid Function Reference Ranges and Determinants: A Literature Overview and a Prospective Cohort Study.Thyroid. 2017 Nov;27(11):1360-1369. doi: 10.1089/thy.2017.0262. Epub 2017 Oct 24. Thyroid. 2017. PMID: 28942709 Review.
Cited by
-
Obstetric and offspring outcomes in isolated maternal hypothyroxinaemia: a systematic review and meta-analysis.J Endocrinol Invest. 2023 Jun;46(6):1087-1101. doi: 10.1007/s40618-022-01967-4. Epub 2022 Nov 23. J Endocrinol Invest. 2023. PMID: 36422828 Free PMC article.
-
Implications of High Free Thyroxine (FT4) concentrations in euthyroid pregnancies: the FaSTER trial.J Clin Endocrinol Metab. 2014 Jun;99(6):2038-44. doi: 10.1210/jc.2014-1053. Epub 2014 Feb 28. J Clin Endocrinol Metab. 2014. PMID: 24606107 Free PMC article.
-
Maternal hypothyroxinaemia in pregnancy is associated with obesity and adverse maternal metabolic parameters.Eur J Endocrinol. 2016 Jan;174(1):51-7. doi: 10.1530/EJE-15-0866. Eur J Endocrinol. 2016. PMID: 26586839 Free PMC article.
-
Association of Thyroid Function Test Values with Prepregnancy Body Mass Index and Gestational Weight Gain: A Systematic Review of Literature Reviews.Iran J Nurs Midwifery Res. 2025 Jan 15;30(1):11-17. doi: 10.4103/ijnmr.ijnmr_274_23. eCollection 2025 Jan-Feb. Iran J Nurs Midwifery Res. 2025. PMID: 40052043 Free PMC article. Review.
-
High Body Mass Index Is an Indicator of Maternal Hypothyroidism, Hypothyroxinemia, and Thyroid-Peroxidase Antibody Positivity during Early Pregnancy.Biomed Res Int. 2015;2015:351831. doi: 10.1155/2015/351831. Epub 2015 Jul 27. Biomed Res Int. 2015. PMID: 26273610 Free PMC article.
References
-
- Andersen S. Bruun NH. Pedersen KM. Laurberg P. Biologic variation is important for interpretation of thyroid function tests. Thyroid. 2003;13:1069–1078. - PubMed
-
- Lambert-Messerlian G. McClain M. Haddow JE. Palomaki GE. Canick JA. Cleary-Goldman J. Malone FD. Porter TF. Nyberg DA. Bernstein P. D'Alton ME. First-, second-trimester thyroid hormone reference data in pregnant women: a FaSTER (First-, Second-Trimester Evaluation of Risk for aneuploidy) Research Consortium study. Am J Obstet Gynecol. 2008;199(62):e61–e66. - PMC - PubMed
-
- Bassols J. Prats-Puig A. Soriano-Rodriguez P. Garcia-Gonzalez MM. Reid J. Martinez-Pascual M. Mateos-Comeron F. de Zegher F. Ibanez L. Lopez-Bermejo A. Lower free thyroxin associates with a less favorable metabolic phenotype in healthy pregnant women. J Clin Endocrinol Metab. 2011;96:3717–3723. - PubMed
-
- Mannisto T. Surcel HM. Ruokonen A. Vaarasmaki M. Pouta A. Bloigu A. Jarvelin MR. Hartikainen AL. Suvanto E. Early pregnancy reference intervals of thyroid hormone concentrations in a thyroid antibody-negative pregnant population. Thyroid. 2011;21:291–298. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
