

The Nigerian antihypertensive adherence trial: a community-based randomized trial
- PMID: 23137954
- PMCID: PMC3530610
- DOI: 10.1097/HJH.0b013e32835b0842
The Nigerian antihypertensive adherence trial: a community-based randomized trial
Abstract
Background: Research in industrialized countries has demonstrated that a key factor limiting the control of hypertension is poor patient adherence and that the most successful interventions for long-term adherence employ multiple strategies. Very little data exist on this question in low-income countries, wherein medication-taking behavior may be less well developed.
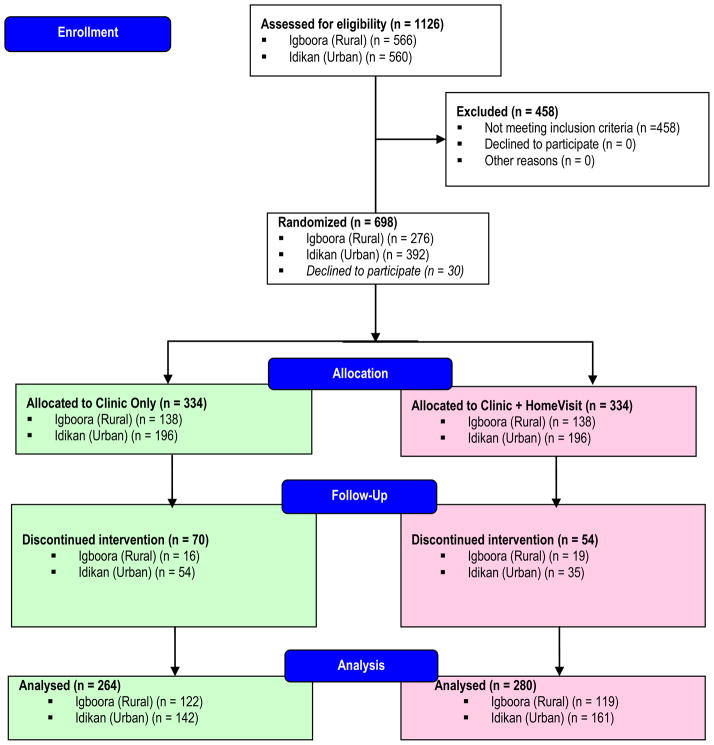
Method: We conducted a treatment adherence trial of 544 patients [mean age ∼63 years, mean blood pressure (BP) ∼168/92 mmHg] with previously untreated hypertension in urban and rural Nigeria. Eligible participants were randomized to one of two arms: clinic management only, or clinic management and home visits. Both interventions included three elements: a community based, nurse-led treatment program with physician backup; facilitation of clinic visits and health education; and the use of diuretics and a β blocker as needed. After initial diagnosis, the management protocol was implemented by a nurse with physician backup. Participants were evaluated monthly for 6 months.
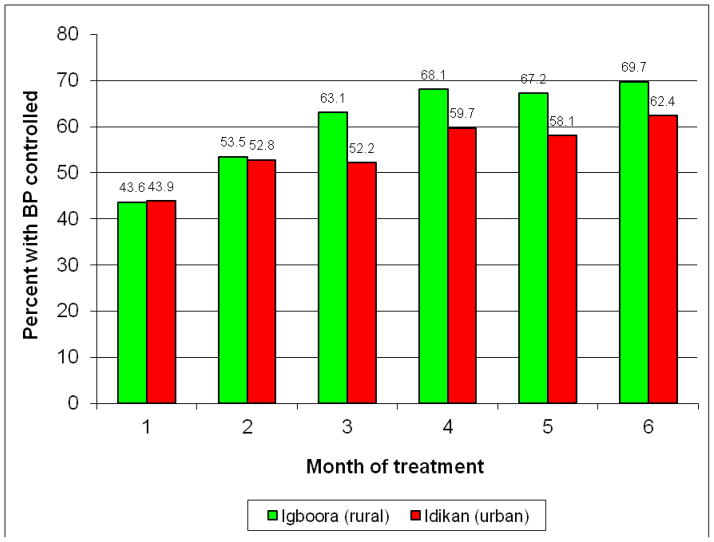
Results: Medication adherence was assessed with pill count and urine testing. Drop-out rates, by treatment group, ranged from 12 to 28%. Among participants who completed the 6-month trial, overall adherence was high (∼77% of participants took >98% of prescribed pills). Adherence did not differ by treatment arm, but was better at the rural than the urban site and among those with higher baseline BP. Hypertension control (BP <140/90 mmHg) was achieved in approximately 66% of participants at 6 months.
Conclusion: This community-based intervention confirms relatively modest default rates compared with industrialized societies, and suggests that medication adherence can be high in developing world settings in clinic attenders.
Conflict of interest statement
Figures

Comment in
-
A community-based intervention program to effectively treat hypertension in developing countries.J Hypertens. 2013 Jan;31(1):47-8. doi: 10.1097/HJH.0b013e32835c7ca0. J Hypertens. 2013. PMID: 23221931 No abstract available.
References
-
- Edwards R, Unwin N, Mugusi F, Whiting D, Rashid S, Kissima J, et al. Hypertension prevalence and care in an urban and rural area of Tanzania. J Hypertens. 2000;18(2):145–52. - PubMed
-
- Fuentes R, Ilmaniemi N, Laurikainen E, Tuomilehto J, Nissinen A. Hypertension in developing economies: a review of population-based studies carried out from 1980 to 1998. J Hypertens. 2000;18(5):521–9. - PubMed
-
- Pobee JO. Community-based high blood pressure programs in sub-Saharan Africa. Ethn Dis. 1993;3(Suppl):S38–45. - PubMed
-
- Walker RW, McLarty DG, Kitange HM, Whiting D, Masuki G, Mtasiwa DM, et al. Stroke mortality in urban and rural Tanzania. Adult Morbidity and Mortality Project. Lancet. 2000;355(9216):1684–7. - PubMed
-
- Arroyo P, Fernandez V, Loria A, Kuri-Morales P, Orozco-Rivadeneyra S, Olaiz G, et al. Hypertension in urban Mexico: the 1992–93 national survey of chronic diseases. J Hum Hypertens. 1999;13(10):671–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
