

Early change in ferumoxytol-enhanced magnetic resonance imaging signal suggests unstable human cerebral aneurysm: a pilot study
- PMID: 23138441
- PMCID: PMC3508354
- DOI: 10.1161/STROKEAHA.112.673400
Early change in ferumoxytol-enhanced magnetic resonance imaging signal suggests unstable human cerebral aneurysm: a pilot study
Abstract
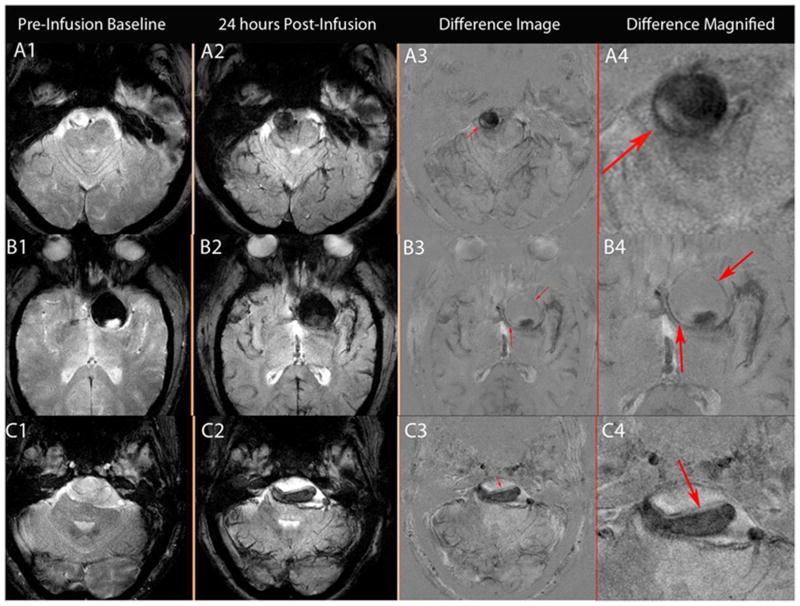
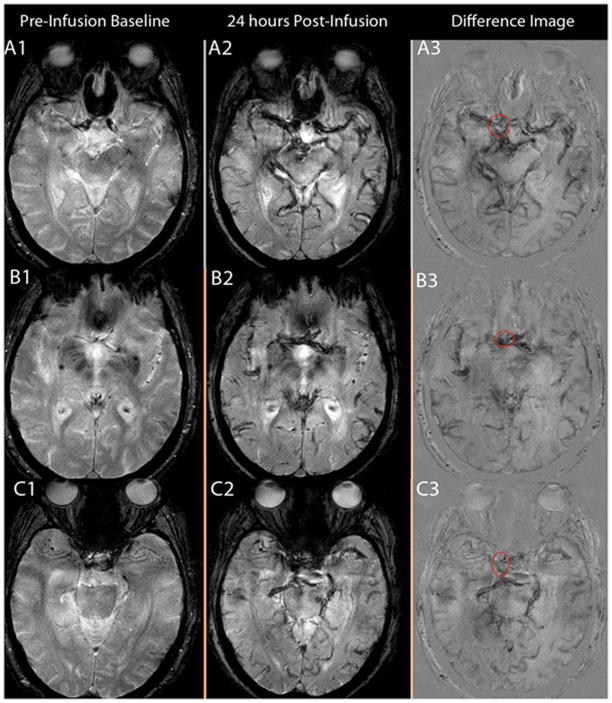
Background and purpose: The clinical significance of early (ie, within the first 24 hours) uptake of ferumoxytol by macrophages in the wall of human cerebral aneurysms is not clear. The purpose of this study was to determine whether early uptake of ferumoxytol suggests unstable cerebral aneurysm.
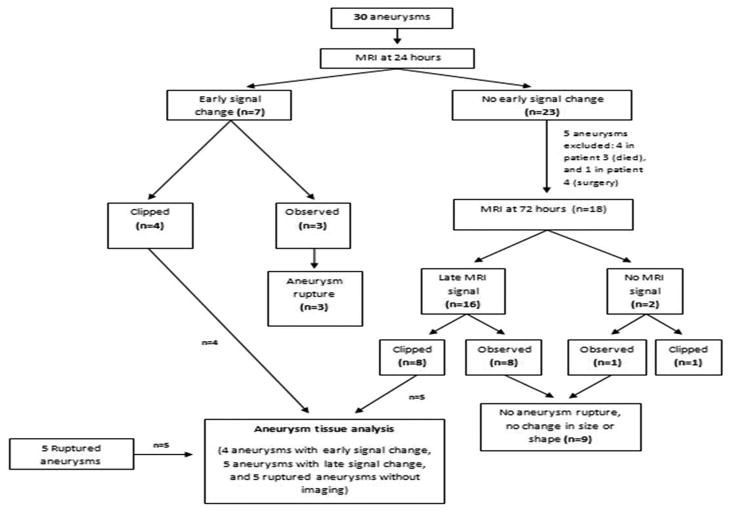
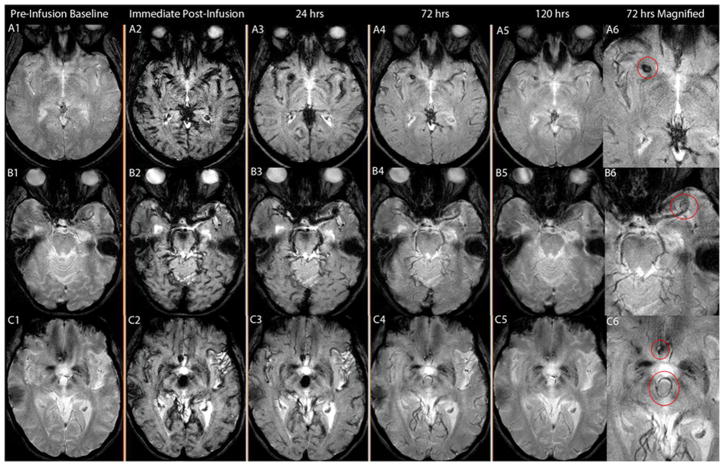
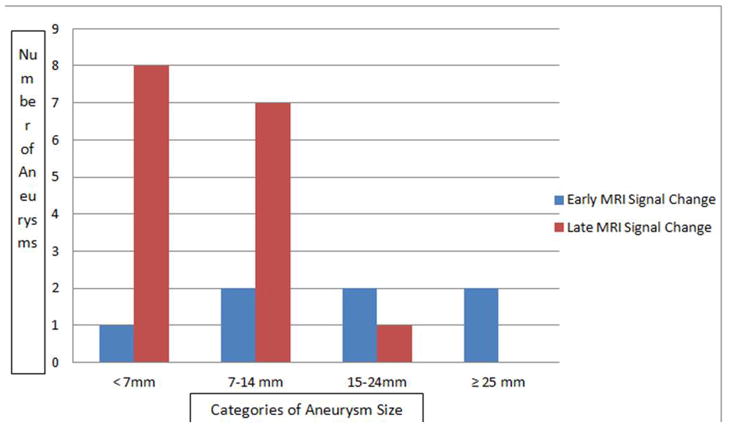
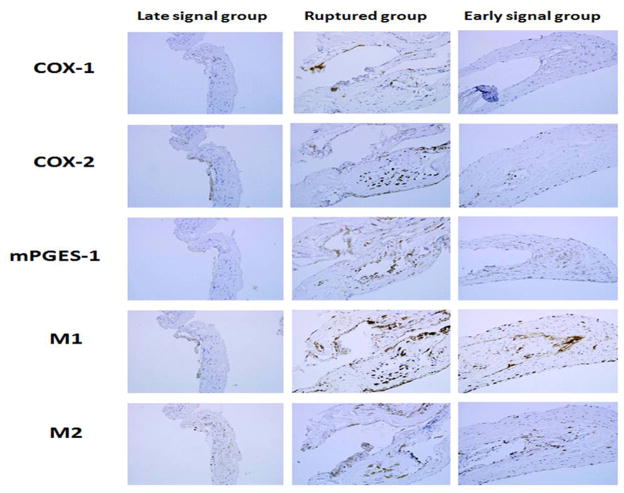
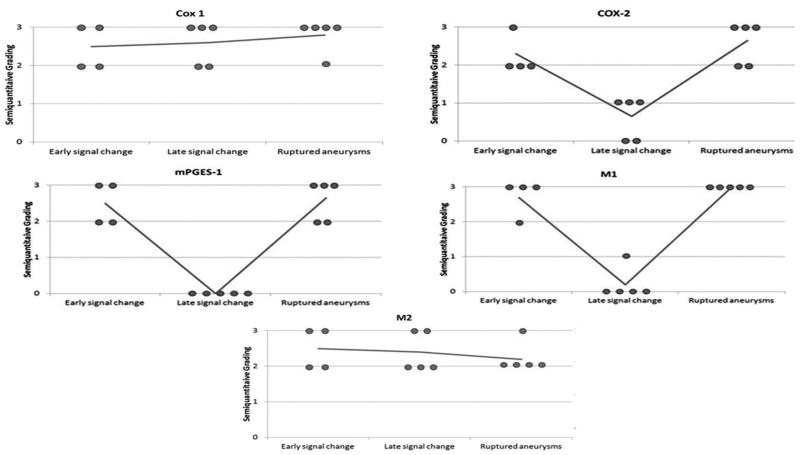
Methods: Thirty unruptured aneurysms in 22 patients were imaged with magnetic resonance imaging 24 hours after infusion of ferumoxytol. Eighteen aneurysms were also imaged 72 hours after infusion of ferumoxytol. Aneurysm dome tissue was collected from 4 patients with early magnetic resonance imaging signal changes, 5 patients with late signal changes, and 5 other patients with ruptured aneurysms. The tissue was immunostained for expression of cyclooxygenase-1, cyclooxygenase-2, microsomal prostaglandin E2 synthase-1, and macrophages.
Results: In 23% (7/30) of aneurysms, there was pronounced early uptake of ferumoxytol. Four aneurysms were clipped. The remaining 3 aneurysms were managed conservatively; all 3 ruptured within 6 months. In 53% (16 of 30) of aneurysms, there was pronounced uptake of ferumoxytol at 72 hours. Eight aneurysms were surgically clipped, and 8 were managed conservatively; none ruptured or increased in size after 6 months. Expression of cyclooxygenase-2, microsomal prostaglandin E2 synthase-1, and macrophages was similar in unruptured aneurysms with early uptake of ferumoxytol and ruptured aneurysms. Expression of these inflammatory molecules was significantly higher in aneurysms with early uptake of ferumoxytol versus aneurysms with late uptake.
Conclusions: Uptake of ferumoxytol in aneurysm walls within the first 24 hours strongly suggests aneurysm instability and probability of rupture within 6 months, and may warrant urgent intervention.
Conflict of interest statement
None
Figures
References
-
- Lu M, Cohen MH, Rieves D, Pazdur R. Fda report: Ferumoxytol for intravenous iron therapy in adult patients with chronic kidney disease. Am J Hematol. 2010;85:315–319. - PubMed
-
- Neuwelt EA, Varallyay CG, Manninger S, Solymosi D, Haluska M, Hunt MA, et al. The potential of ferumoxytol nanoparticle magnetic resonance imaging, perfusion, and angiography in central nervous system malignancy: A pilot study. Neurosurgery. 2007;60:601–611. discussion 611-602. - PubMed
-
- Herborn CU, Vogt FM, Lauenstein TC, Dirsch O, Corot C, Robert P, et al. Magnetic resonance imaging of experimental atherosclerotic plaque: Comparison of two ultrasmall superparamagnetic particles of iron oxide. J Magn Reson Imaging. 2006;24:388–393. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
