

Circulating suPAR in two cohorts of primary FSGS
- PMID: 23138488
- PMCID: PMC3507361
- DOI: 10.1681/ASN.2012030302
Circulating suPAR in two cohorts of primary FSGS
Abstract
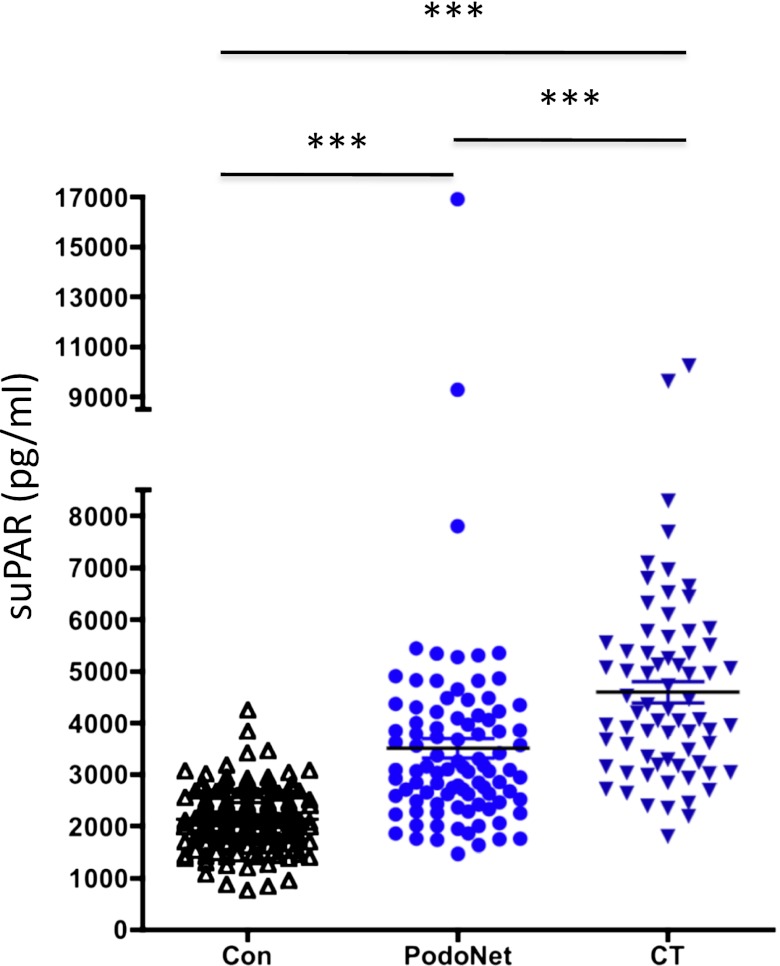
Overexpression of soluble urokinase receptor (suPAR) causes pathology in animal models similar to primary FSGS, and one recent study demonstrated elevated levels of serum suPAR in patients with the disease. Here, we analyzed circulating suPAR levels in two cohorts of children and adults with biopsy-proven primary FSGS: 70 patients from the North America-based FSGS clinical trial (CT) and 94 patients from PodoNet, the Europe-based consortium studying steroid-resistant nephrotic syndrome. Circulating suPAR levels were elevated in 84.3% and 55.3% of patients with FSGS patients in the CT and PodoNet cohorts, respectively, compared with 6% of controls (P<0.0001); inflammation did not account for this difference. Multiple regression analysis suggested that lower suPAR levels associated with higher estimated GFR, male sex, and treatment with mycophenolate mofetil. In the CT cohort, there was a positive association between the relative reduction of suPAR after 26 weeks of treatment and reduction of proteinuria, with higher odds for complete remission (P=0.04). In the PodoNet cohort, patients with an NPHS2 mutation had higher suPAR levels than those without a mutation. In conclusion, suPAR levels are elevated in geographically and ethnically diverse patients with FSGS and do not reflect a nonspecific proinflammatory milieu. The associations between a change in circulating suPAR with different therapeutic regimens and with remission support the role of suPAR in the pathogenesis of FSGS.
Figures



Comment in
-
Glomerular disease: 'suPAR'-exciting times for FSGS.Nat Rev Nephrol. 2013 Mar;9(3):127-8. doi: 10.1038/nrneph.2013.15. Epub 2013 Feb 5. Nat Rev Nephrol. 2013. PMID: 23381372 No abstract available.
References
-
- Benchimol C: Focal segmental glomerulosclerosis: Pathogenesis and treatment. Curr Opin Pediatr 15: 171–180, 2003 - PubMed
-
- Korbet SM: Treatment of primary focal segmental glomerulosclerosis. Kidney Int 62: 2301–2310, 2002 - PubMed
-
- Boyer O, Moulder JK, Somers MJ: Focal and segmental glomerulosclerosis in children: A longitudinal assessment. Pediatr Nephrol 22: 1159–1166, 2007 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
