

Focal peliosis hepatis in a colon cancer patient resembling metastatic liver tumor
- PMID: 23139621
- PMCID: PMC3491612
- DOI: 10.3748/wjg.v18.i41.5999
Focal peliosis hepatis in a colon cancer patient resembling metastatic liver tumor
Abstract
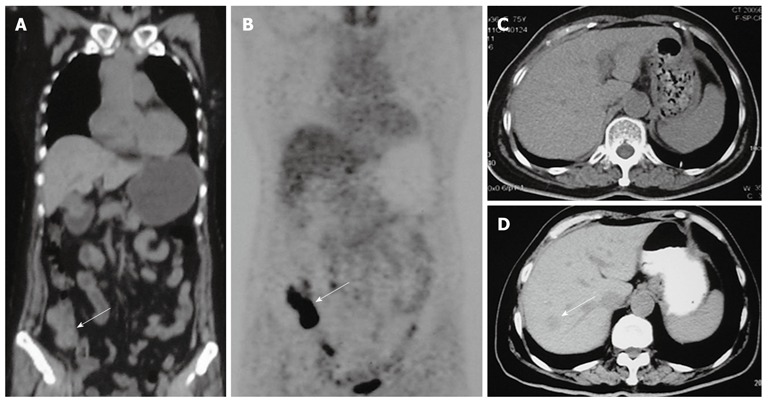
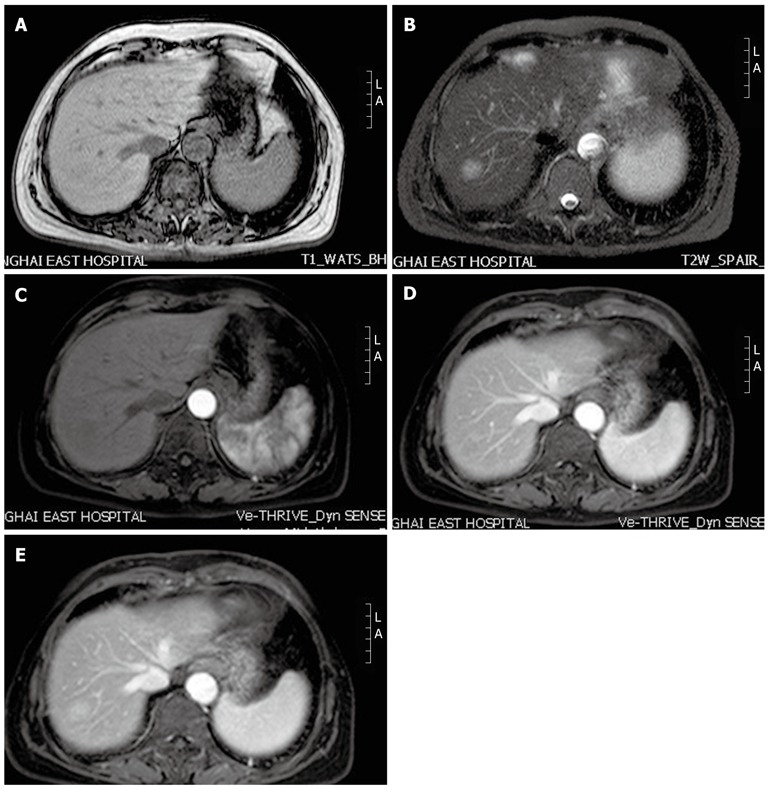
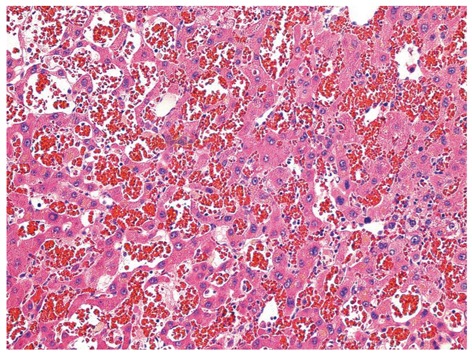
Peliosis hepatis (PH) is a rare benign condition characterized by the presence of multiple, randomly distributed, blood filled cystic areas of variable size within the liver parenchyma. PH is difficult to recognize and may be mistaken for neoplasm, metastases or multiple abscesses. A 75-year-old female with a previous history of colon cancer was admitted when a liver mass in the right liver lobe was found 11 mo after surgery during the follow-up period. Computed tomography and magnetic resonance imaging scan of the abdomen were performed. The initial possible diagnosis was metastatic hepatocellular carcinoma. The patient underwent excision of the hepatic segment where the nodule was located. The pathological diagnosis of the surgical specimen was PH. PH should be considered in the differential diagnosis of new liver lesions in patients whose clinical settings do not clearly favor metastasization. Clinicians and radiologists must recognize these lesions to minimize the probability of misdiagnosis and inappropriate treatment.
Keywords: Differential diagnosis; Metastatic liver tumor; Peliosis hepatis.
Figures
References
-
- Tsokos M, Erbersdobler A. Pathology of peliosis. Forensic Sci Int. 2005;149:25–33. - PubMed
-
- Biswas S, Rolain JM. Bartonella infection: treatment and drug resistance. Future Microbiol. 2010;5:1719–1731. - PubMed
-
- Sandrasegaran K, Hawes DR, Matthew G. Hepatic peliosis (bacillary angiomatosis) in AIDS: CT findings. Abdom Imaging. 2005;30:738–740. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
