

A novel low-energy electrotherapy that terminates ventricular tachycardia with lower energy than a biphasic shock when antitachycardia pacing fails
- PMID: 23141483
- PMCID: PMC4573535
- DOI: 10.1016/j.jacc.2012.08.1001
A novel low-energy electrotherapy that terminates ventricular tachycardia with lower energy than a biphasic shock when antitachycardia pacing fails
Abstract
Objectives: The authors sought to develop a low-energy electrotherapy that terminates ventricular tachycardia (VT) when antitachycardia pacing (ATP) fails.
Background: High-energy implantable cardioverter-defibrillator (ICD) shocks are associated with device failure, significant morbidity, and increased mortality. A low-energy alternative to ICD shocks is desirable.
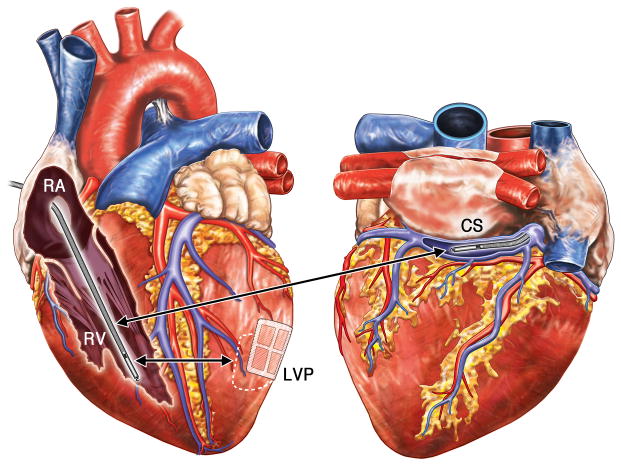
Methods: Myocardial infarction was created in 25 dogs. Sustained, monomorphic VT was induced by programmed stimulation. Defibrillation electrodes were placed in the right ventricular apex, and coronary sinus and left ventricular epicardium. If ATP failed to terminate sustained VT, the defibrillation thresholds (DFTs) of standard versus experimental electrotherapies were measured.
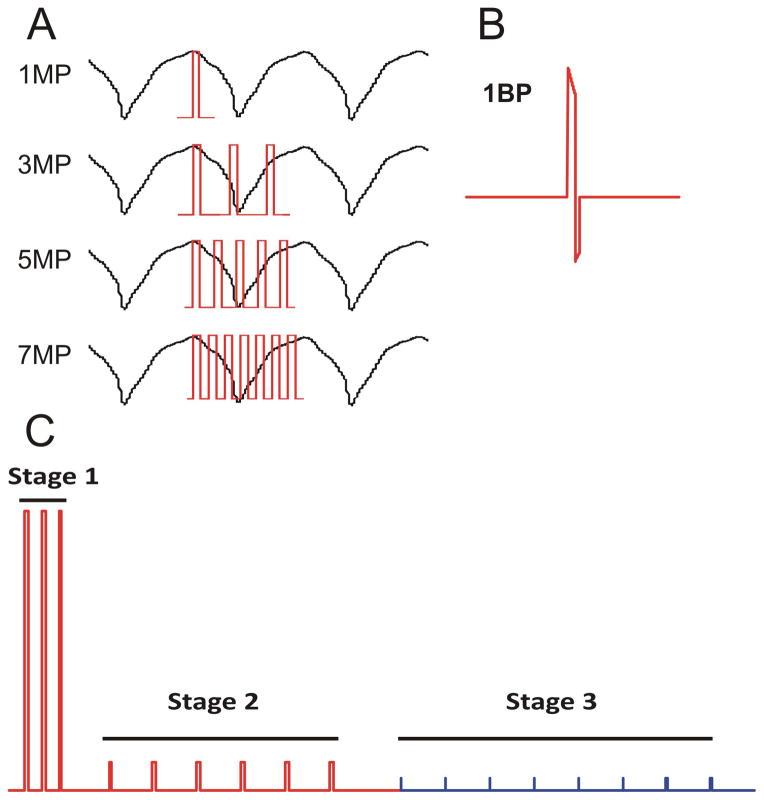
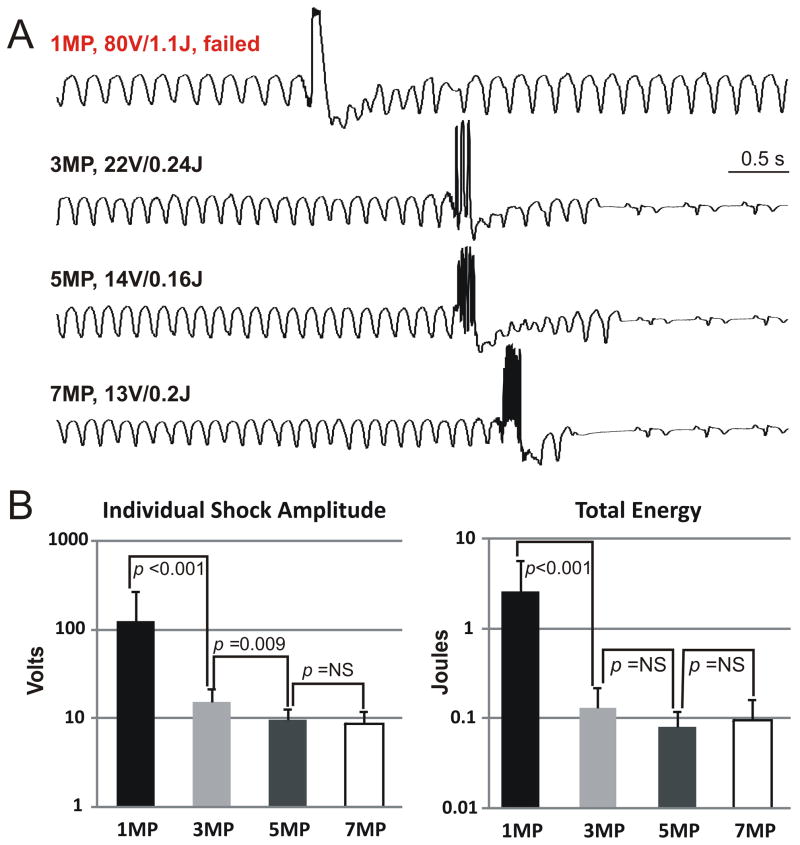
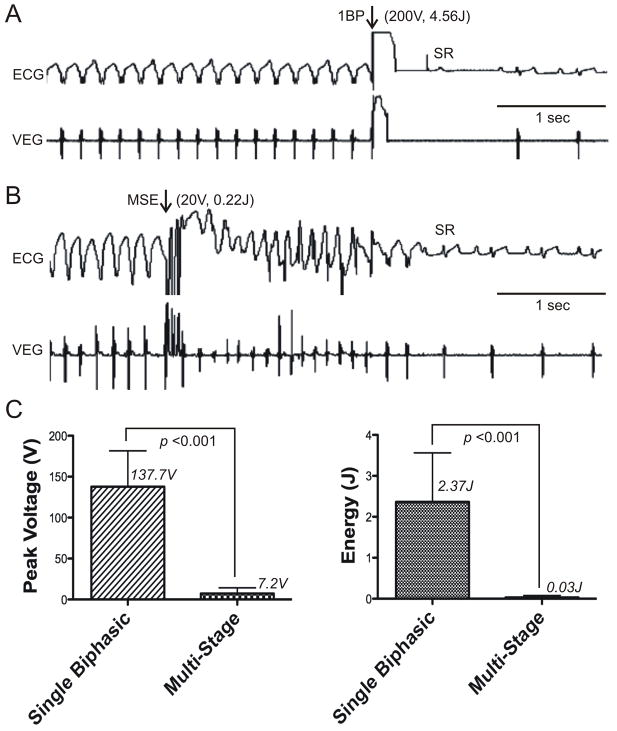
Results: Sustained VT ranged from 276 to 438 beats/min (mean 339 beats/min). The right ventricular-coronary sinus shock vector had lower impedance than the right ventricular-left ventricular patch (54.4 ± 18.1 Ω versus 109.8 ± 16.9 Ω; p < 0.001). A single shock required between 0.3 ± 0.2 J to 5.9 ± 2.5 J (mean 2.64 ± 3.22 J; p = 0.008) to terminate VT, and varied depending upon the phase of the VT cycle in which it was delivered. By contrast, multiple shocks delivered within 1 VT cycle length were not phase dependent and achieved lower DFT compared with a single shock (0.13 ± 0.09 J for 3 shocks, 0.08 ± 0.04 J for 5 shocks, and 0.09 ± 0.07 J for 7 shocks; p < 0.001). Finally, a multistage electrotherapy (MSE) achieved significantly lower DFT compared with a single biphasic shock (0.03 ± 0.05 J versus 2.37 ± 1.20 J; respectively, p < 0.001). At a peak shock amplitude of 20 V, MSE achieved 91.3% of terminations versus 10.5% for a biphasic shock (p < 0.001).
Conclusions: MSE achieved a major reduction in DFT compared with a single biphasic shock for ATP-refractory monomorphic VT, and represents a novel electrotherapy to reduce high-energy ICD shocks.
Copyright © 2012 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Evolution of the implantable cardioverter-defibrillator: from bullets to BBs.J Am Coll Cardiol. 2012 Dec 11;60(23):2399-401. doi: 10.1016/j.jacc.2012.07.066. Epub 2012 Nov 7. J Am Coll Cardiol. 2012. PMID: 23141489 No abstract available.
References
-
- Moss AJ, Hall WJ, Cannom DS, et al. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. Multicenter Automatic Defibrillator Implantation Trial Investigators N Engl J Med. 1996;335:1933–40. - PubMed
-
- Buxton AE, Lee KL, Fisher JD, Josephson ME, Prystowsky EN, Hafley G. A randomized study of the prevention of sudden death in patients with coronary artery disease. Multicenter Unsustained Tachycardia Trial Investigators N Engl J Med. 1999;341:1882–90. - PubMed
-
- Zipes DP, Wellens HJ. Sudden cardiac death. Circulation. 1998;98:2334–51. - PubMed
-
- Schron EB, Exner DV, Yao Q, et al. Quality of life in the antiarrhythmics versus implantable defibrillators trial: impact of therapy and influence of adverse symptoms and defibrillator shocks. Circulation. 2002;105:589–94. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
