

Clinical significance and developmental changes of auditory-language-related gamma activity
- PMID: 23141882
- PMCID: PMC3577943
- DOI: 10.1016/j.clinph.2012.09.031
Clinical significance and developmental changes of auditory-language-related gamma activity
Abstract
Objective: We determined the clinical impact and developmental changes of auditory-language-related augmentation of gamma activity at 50-120 Hz recorded on electrocorticography (ECoG).
Methods: We analyzed data from 77 epileptic patients ranging 4-56 years in age. We determined the effects of seizure-onset zone, electrode location, and patient-age upon gamma-augmentation elicited by an auditory-naming task.
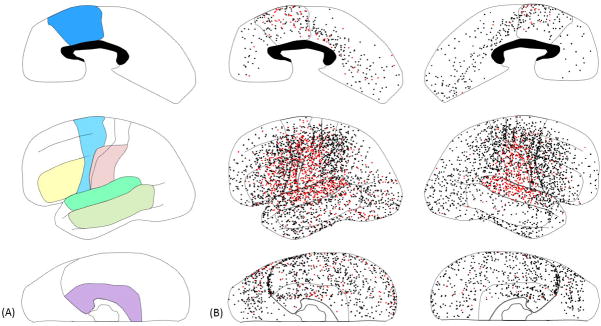
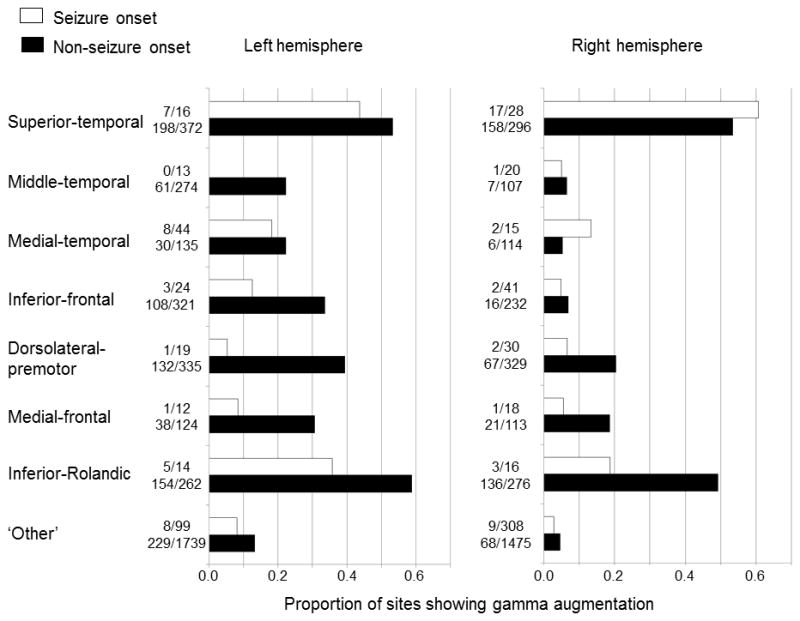
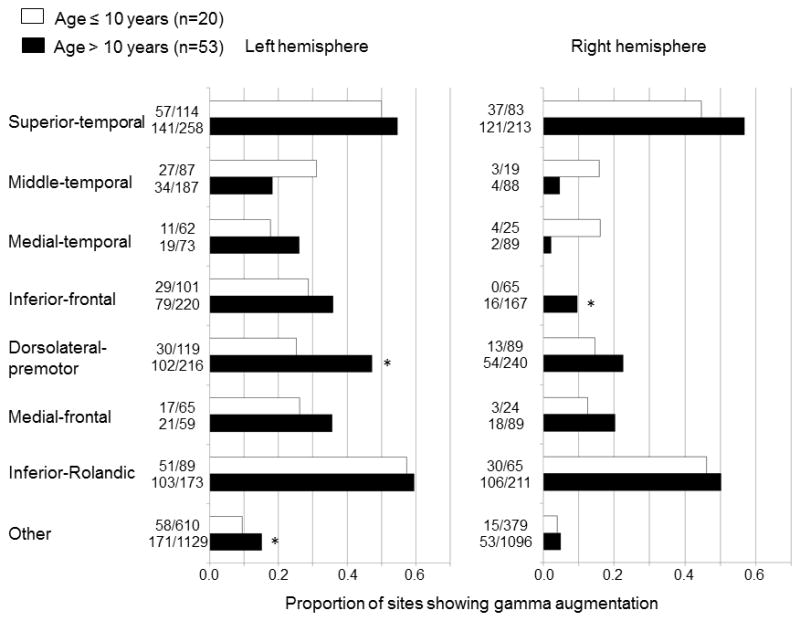
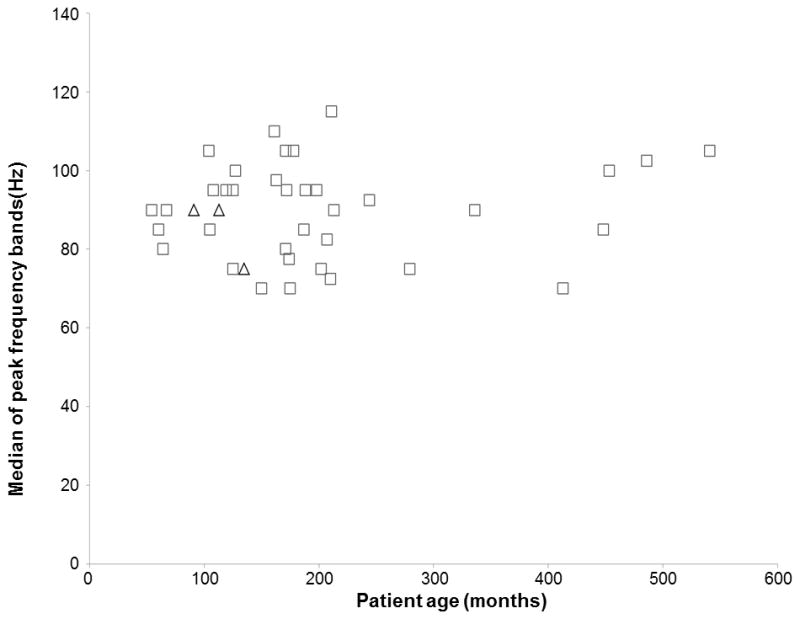
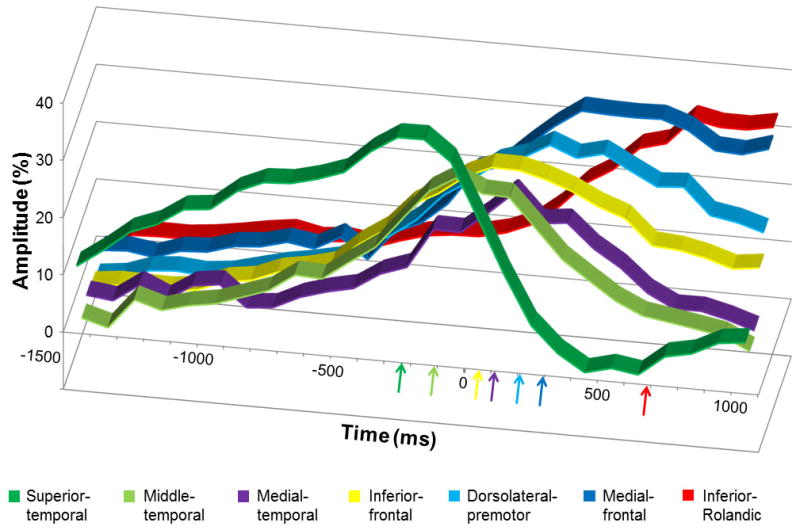
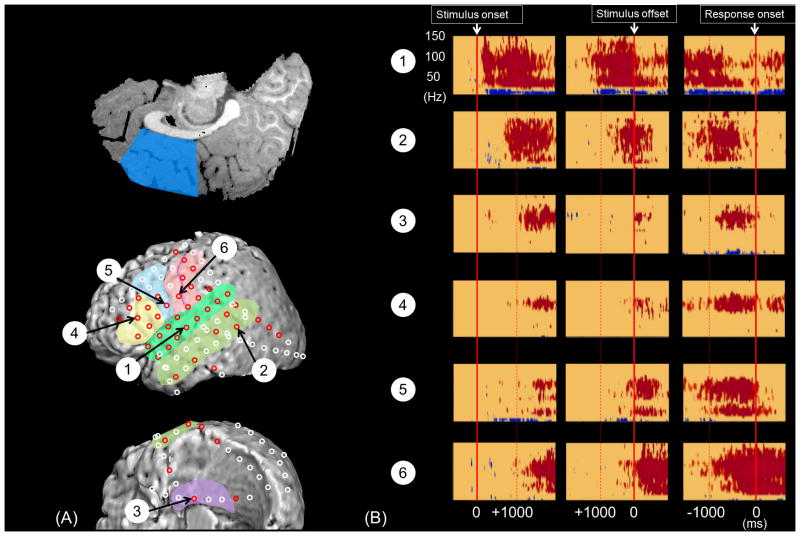
Results: Gamma-augmentation was less frequently elicited within seizure-onset sites compared to other sites. Regardless of age, gamma-augmentation most often involved the 80-100 Hz frequency band. Gamma-augmentation initially involved bilateral superior-temporal regions, followed by left-side dominant involvement in the middle-temporal, medial-temporal, inferior-frontal, dorsolateral-premotor, and medial-frontal regions and concluded with bilateral inferior-Rolandic involvement. Compared to younger patients, those older than 10 years had a larger proportion of left dorsolateral-premotor and right inferior-frontal sites showing gamma-augmentation. The incidence of a post-operative language deficit requiring speech therapy was predicted by the number of resected sites with gamma-augmentation in the superior-temporal, inferior-frontal, dorsolateral-premotor, and inferior-Rolandic regions of the left hemisphere assumed to contain essential language function (r(2) = 0.59; p = 0.001; odds ratio = 6.04 [95% confidence-interval: 2.26-16.15]).
Conclusions: Auditory-language-related gamma-augmentation can provide additional information useful to localize the primary language areas.
Significance: These results derived from a large sample of patients support the utility of auditory-language-related gamma-augmentation in presurgical evaluation.
Copyright © 2012 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights reserved.
Figures
Comment in
-
Does measurement of event-related gamma-augmentation replace electrical stimulation via intracranial electrodes?Clin Neurophysiol. 2013 May;124(5):829-30. doi: 10.1016/j.clinph.2012.10.010. Epub 2012 Nov 8. Clin Neurophysiol. 2013. PMID: 23141883 No abstract available.
Similar articles
-
Gamma activity modulated by picture and auditory naming tasks: intracranial recording in patients with focal epilepsy.Clin Neurophysiol. 2013 Sep;124(9):1737-44. doi: 10.1016/j.clinph.2013.01.030. Epub 2013 May 18. Clin Neurophysiol. 2013. PMID: 23688918 Free PMC article.
-
Three- and four-dimensional mapping of speech and language in patients with epilepsy.Brain. 2017 May 1;140(5):1351-1370. doi: 10.1093/brain/awx051. Brain. 2017. PMID: 28334963 Free PMC article.
-
Four-dimensional functional cortical maps of visual and auditory language: Intracranial recording.Epilepsia. 2019 Feb;60(2):255-267. doi: 10.1111/epi.14648. Epub 2019 Feb 1. Epilepsia. 2019. PMID: 30710356 Free PMC article.
-
Multimodality language mapping in patients with left-hemispheric language dominance on Wada test.Clin Neurophysiol. 2012 Oct;123(10):1917-24. doi: 10.1016/j.clinph.2012.01.027. Epub 2012 Apr 12. Clin Neurophysiol. 2012. PMID: 22503906 Free PMC article.
-
Presurgical language mapping using event-related high-gamma activity: The Detroit procedure.Clin Neurophysiol. 2018 Jan;129(1):145-154. doi: 10.1016/j.clinph.2017.10.018. Epub 2017 Oct 31. Clin Neurophysiol. 2018. PMID: 29190521 Free PMC article. Review.
Cited by
-
Objective Detection of Eloquent Axonal Pathways to Minimize Postoperative Deficits in Pediatric Epilepsy Surgery using Diffusion Tractography and Convolutional Neural Networks.IEEE Trans Med Imaging. 2019 Feb 27:10.1109/TMI.2019.2902073. doi: 10.1109/TMI.2019.2902073. Online ahead of print. IEEE Trans Med Imaging. 2019. PMID: 30835220 Free PMC article.
-
Electrocorticographic correlates of overt articulation of 44 English phonemes: intracranial recording in children with focal epilepsy.Clin Neurophysiol. 2014 Jun;125(6):1129-37. doi: 10.1016/j.clinph.2013.11.008. Epub 2013 Nov 19. Clin Neurophysiol. 2014. PMID: 24315545 Free PMC article. Clinical Trial.
-
Long-term satisfaction after extraoperative invasive EEG recording.Epilepsy Behav. 2021 Oct 27;124:108363. doi: 10.1016/j.yebeh.2021.108363. Epub 2021 Oct 27. Epilepsy Behav. 2021. PMID: 34717248 Free PMC article.
-
Characterizing physiological high-frequency oscillations using deep learning.J Neural Eng. 2022 Dec 7;19(6):10.1088/1741-2552/aca4fa. doi: 10.1088/1741-2552/aca4fa. J Neural Eng. 2022. PMID: 36541546 Free PMC article.
-
Contribution of research on 'Epilepsy & behavior' to the refinement of functional brain atlas in four dimensions.Epilepsy Behav. 2014 Nov;40:86-8. doi: 10.1016/j.yebeh.2014.08.030. Epub 2014 Sep 26. Epilepsy Behav. 2014. PMID: 25262069 Free PMC article.
References
-
- Adleman NE, Menon V, Blasey CM, White CD, Warsofsky IS, Glover GH, Reiss AL. A developmental fMRI study of the Stroop color-word task. Neuroimage. 2002;16:61–75. - PubMed
-
- Akanuma N, Alarcón G, Lum F, Kissani N, Koutroumanidis M, Adachi N, et al. Lateralising value of neuropsychological protocols for presurgical assessment of temporal lobe epilepsy. Epilepsia. 2003;44:408–418. - PubMed
-
- Akiyama T, McCoy B, Go CY, Ochi A, Elliott IM, Akiyama M, et al. Focal resection of fast ripples on extraoperative intracranial EEG improves seizure outcome in pediatric epilepsy. Epilepsia. 2011;52:1802–11. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
