

Effective antimicrobial stewardship in a long-term care facility through an infectious disease consultation service: keeping a LID on antibiotic use
- PMID: 23143354
- PMCID: PMC4370223
- DOI: 10.1086/668429
Effective antimicrobial stewardship in a long-term care facility through an infectious disease consultation service: keeping a LID on antibiotic use
Abstract
Design: We introduced a long-term care facility (LTCF) infectious disease (ID) consultation service (LID service) that provides on-site consultations to residents of a Veterans Affairs (VA) LTCF. We determined the impact of the LID service on antimicrobial use and Clostridium difficile infections at the LTCF.
Setting: A 160-bed VA LTCF.
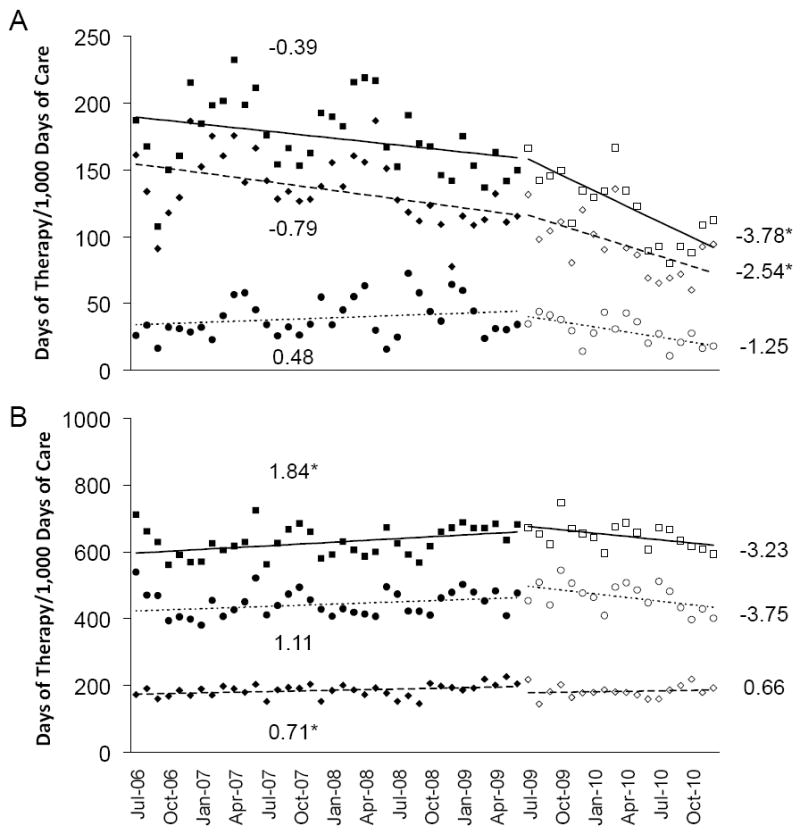
Methods: Systemic antimicrobial use and positive C. difficile tests at the LTCF were compared for the 36 months before and the 18 months after the initiation of the ID consultation service through segmented regression analysis of an interrupted time series.
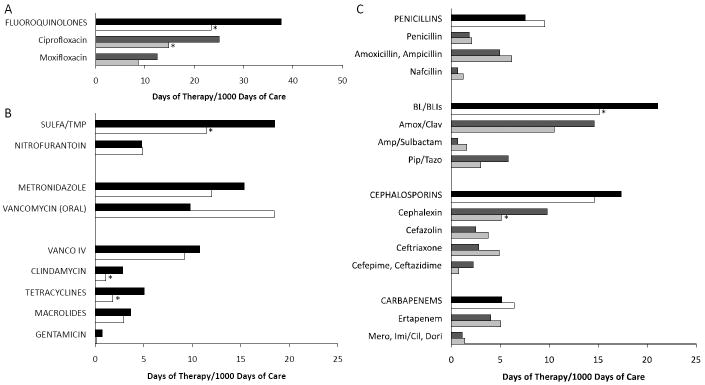
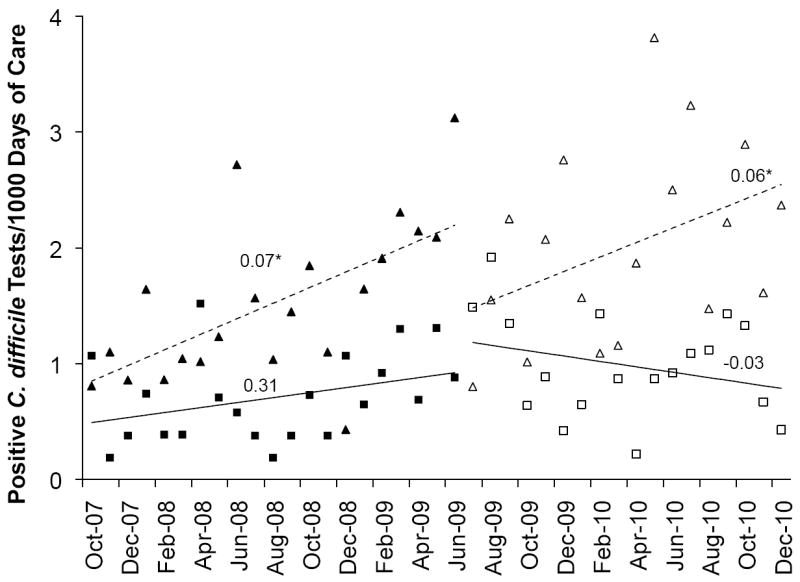
Results: Relative to that in the preintervention period, total systemic antibiotic administration decreased by 30% (P<.001), with significant reductions in both oral (32%; P<.001) and intravenous (25%; P=.008) agents. The greatest reductions were seen for tetracyclines (64%; P<.001), clindamycin (61%; P<.001), sulfamethoxazole/trimethoprim (38%; P<.001), fluoroquinolones (38%; P<.001), and β-lactam/β-lactamase inhibitor combinations (28%; P<.001). The rate of positive C. difficile tests at the LTCF declined in the postintervention period relative to preintervention rates (P=.04).
Conclusions: Implementation of an LTCF ID service led to a significant reduction in total antimicrobial use. Bringing providers with ID expertise to the LTCF represents a new and effective means to achieve antimicrobial stewardship.
Conflict of interest statement
RLPJ reports having consulted for GOJO and Pfizer and has received grant support from Steris, Merck and ViroPharma. RAB reports having consulted for AstraZeneca and having received grant support from AstraZeneca, Ribx, Pfizer and Steris. CJD reports having consulted for BioK, Optimer and GOJO and has received grant support from ViroPharma, Merck and Pfizer. All remaining authors report no conflicts of interest relevant to this article. All authors submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest, and the conflicts that the editors consider relevant to this article are disclosed here.
Figures
References
-
- Jones AL, Dwyer LL, Bercovitz AR, Strahan GW. The National Nursing Home Survey: 2004 overview. Vital Health Stat. 2009;13(167):1–155. - PubMed
-
- Anon. Health, United States, 2010: With Special Feature on Death and Dying. Hyattsville, MD: National Center for Heatlh Statistics; 2011. - PubMed
-
- US Census Bureau Public Information Office. [March 7th, 2012];US Census Bureau Newsroom: Population: An Older and More Diverse Nation by Midcentury. 2008 http://www.census.gov/newsroom/releases/archives/population/cb08-123.html.
-
- Strausbaugh LJ, Joseph CL. The burden of infection in long-term care. Infect Control Hosp Epidemiol. 2000;21(10):674–679. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
