

Obesity in children with poorly controlled asthma: Sex differences
- PMID: 23143849
- PMCID: PMC3578966
- DOI: 10.1002/ppul.22707
Obesity in children with poorly controlled asthma: Sex differences
Abstract
Background: Obesity increases asthma risk, and may alter asthma severity. In adults, sex appears to modify the effect of obesity on asthma. Among children, the effect of sex on the relationship between obesity and asthma severity remains less clear, particularly when considering race.
Objective: To determine how obesity affects disease characteristics in a diverse cohort of children with poorly controlled asthma, and if obesity effects are altered by sex.
Design: We analyzed 306 children between 6 and 17 years of age with poorly controlled asthma enrolled in a 6-month trial assessing lansoprazole for asthma control. In this secondary analysis, we determined associations between obesity and symptom severity, spirometry, exacerbation risk, airway biomarkers, bronchial reactivity, and airflow perception. We used both a multivariate linear regression and longitudinal mixed-effect model to determine if obesity interacted with sex to affect asthma severity.
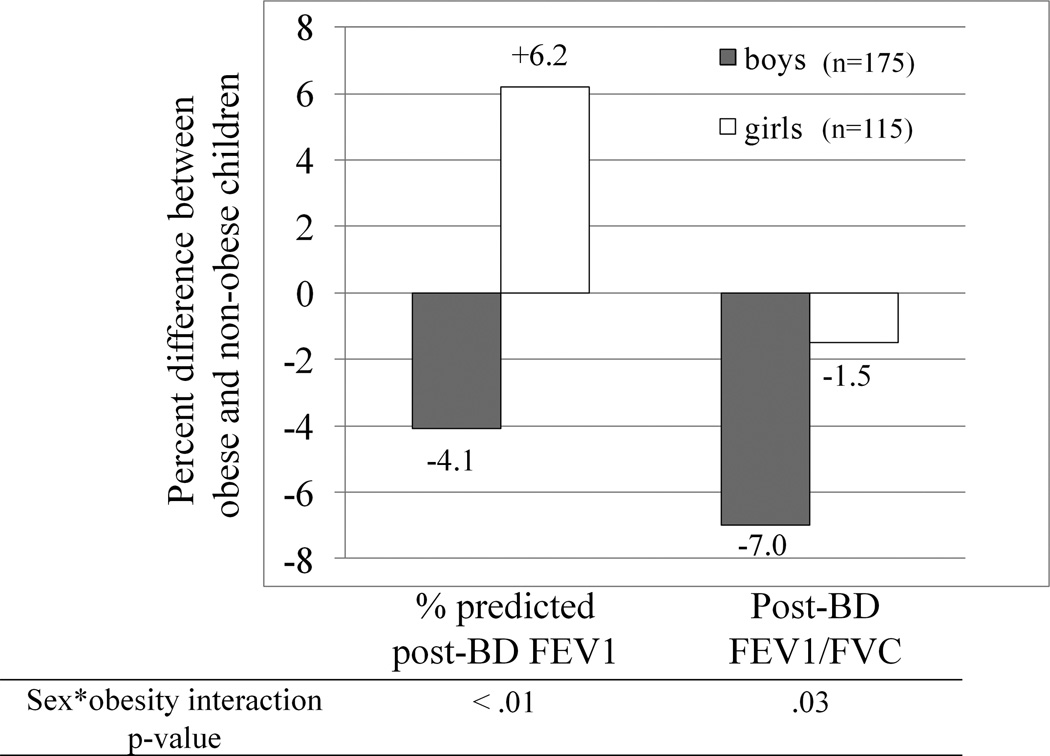
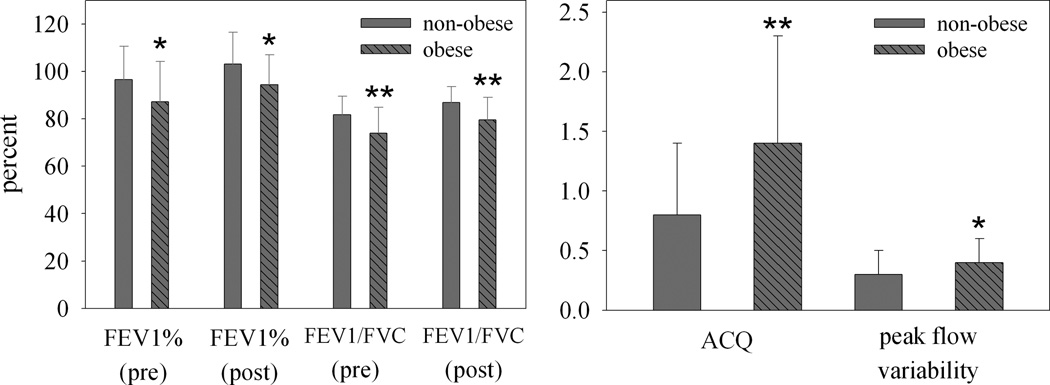
Results: Regardless of sex, BMI >95th percentile did not affect asthma control, exacerbation risk or airway biomarkers. Sex changed the effect of obesity on lung function (sex × obesity FEV1%, interaction P-value < 0.01, sex × obesity FEV1/FVC, interaction P-value = 0.03). Obese males had significantly worse airflow obstruction compared to non-obese males, while in females there was no obesity effect on airflow obstruction. In females, obesity was associated with significantly greater FEV1 and FVC, and a trend toward reduced airway reactivity.
Conclusions: Obesity did not affect asthma control, airway markers or disease stability; however obesity did affect lung function in a sex-dependent manner. In males, obesity associated with reduced FEV1/FVC, and in females, obesity associated with substantially improved lung function.
Keywords: asthma; body mass index; children; obesity; sex; spirometry.
Copyright © 2012 Wiley Periodicals, Inc.
Conflict of interest statement
Dr. Lang has no conflicts of interest in the subject matter of this manuscript
Dr. Holbrook has no conflicts of interest in the subject matter of this manuscript
Dr. Wise has no conflicts of interest in the subject matter of this manuscript
Dr. Dixon has no conflicts of interest in the subject matter of this manuscript
Dr. Teague has no conflicts of interest in the subject matter of this manuscript
Ms. Wei has no conflicts of interest in the subject matter of this manuscript
Dr. Irvin has no conflicts of interest in the subject matter of this manuscript
Dr. Shade as no conflicts of interest in the subject matter of this manuscript
Dr. Lima has no conflicts of interest in the subject matter of this manuscript
Figures
References
-
- Lotvall J, Akdis CA, Bacharier LB, Bjermer L, Casale TB, Custovic A, Lemanske RF, Jr, Wardlaw AJ, Wenzel SE, Greenberger PA. Asthma endotypes: a new approach to classification of disease entities within the asthma syndrome. J Allergy Clin Immunol. 2011;127(2):355–360. - PubMed
-
- Lang JE, Hossain J, Dixon AE, Shade D, Wise RA, Peters SP, Lima JJ. Does age impact the obese asthma phenotype? Longitudinal asthma control, airway function, and airflow perception among mild persistent asthmatics. Chest. 2011;140(6):1524–1533. - PubMed
-
- Castro-Rodriguez JA, Holberg CJ, Morgan WJ, Wright AL, Martinez FD. Increased incidence of asthmalike symptoms in girls who become overweight or obese during the school years. Am J Respir Crit Care Med. 2001;163(6):1344–1349. - PubMed
