

Regional and temporal variation in the treatment of rheumatoid arthritis across the UK: a descriptive register-based cohort study
- PMID: 23144258
- PMCID: PMC3533005
- DOI: 10.1136/bmjopen-2012-001603
Regional and temporal variation in the treatment of rheumatoid arthritis across the UK: a descriptive register-based cohort study
Abstract
Objectives: To describe current disease-modifying antirheumatic drugs (DMARDs) prescription in rheumatoid arthritis (RA) with reference to best practice and to identify temporal and regional trends in the UK.
Design: Descriptive, register-based cohort study.
Participants: Permanently registered patients aged ≥18 years with a recorded diagnosis of RA between 1 January 1995 and 31 March 2010 and matched controls. Participants with RA were identified through screening of all patients in the General Practice Research Database (GPRD) with a clinical or referral record for RA and at least 1 day of follow-up.
Setting: 639 general practices in the UK supplying data to the GPRD.
Main outcome measures: Medication prescribing between 3 and 12 months of RA diagnosis by region and time period (1995-1999, 2000-2005 and 2006-April 2010).
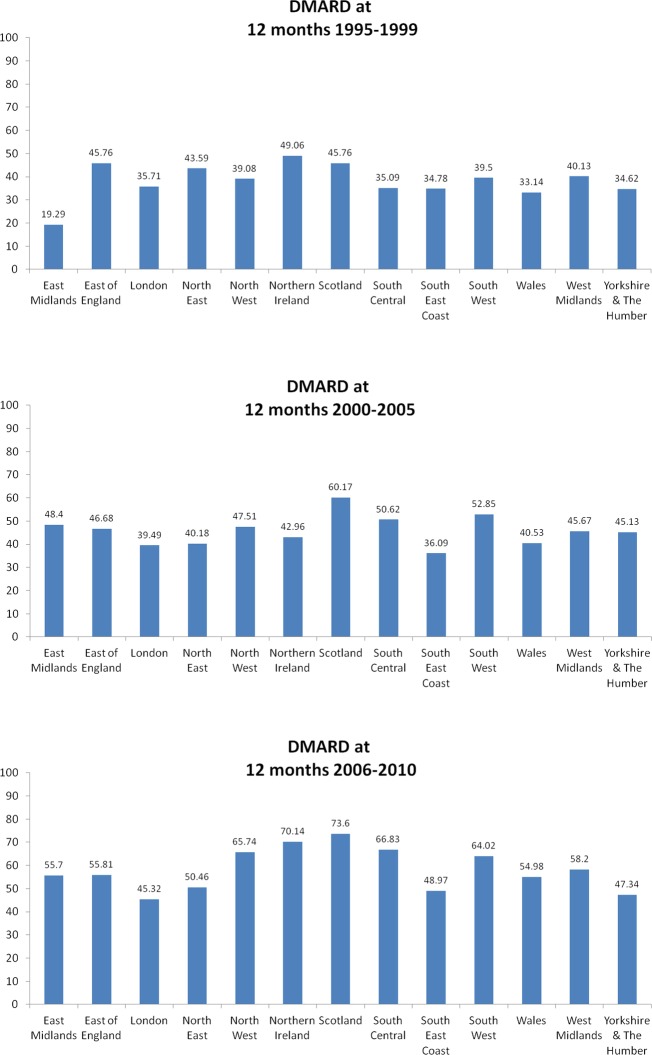
Results: Of the 35 911 patients in the full RA cohort, 15 259 patients (42%) had incident RA. Analysis of prescribing in incident RA patients demonstrated that between 1995 (baseline) and 2010 there was a substantial increase in DMARD, and specifically methotrexate, prescribing across all regions with a less marked increase in combination DMARD prescribing. Taking 12-month prescribing as a snapshot: DMARD prescribing was 19-49% at baseline increasing to 45-74% by 2006-April 2010; methotrexate prescribing was 4-16% at baseline increasing to 32-60%; combination DMARD prescribing was 0-8% at baseline increasing to 3-17%. However, there was marked regional variation in the proportion of RA patients receiving DMARD regardless of time period.
Conclusions: There has been a substantial increase in prescribing of DMARDs for RA since 1995; however, regional variation persists across the UK with relative undertreatment, according to established best practice. Improved implementation of evidence-based best clinical practice to facilitate removal of treatment variation is warranted. This may occur as a result of the implementation of published national guidance.
Figures
References
-
- Choy EH, Panayi GS. Cytokine pathways and joint inflammation in rheumatoid arthritis. N Engl J Med 2001;344:907–16 - PubMed
-
- Wong JB, Ramey DR, Singh G. Long-term morbidity, mortality, and economics of rheumatoid arthritis. Arthritis Rheum 2001;44:2746–9 - PubMed
-
- NAO 2009. National Audit Offices. Services for people with rheumatoid arthritis. The Stationary Office. www.nao.org.uk/publications/0809/services_for_people_with_rheum.aspx (accessed Apr 2012)
-
- Ovayolu N, Ovayolu O, Karadag G. Health-related quality of life in ankylosing spondylitis, fibromyalgia syndrome, and rheumatoid arthritis: a comparison with a selected sample of healthy individuals. Clin Rheumatol 2011;30:655–64 - PubMed
-
- Fleischmann R. Don't forget traditional DMARDs. Old friends are still useful. Rheumatology 2011;50:429–30 - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous