

Clinical value of prognosis gene expression signatures in colorectal cancer: a systematic review
- PMID: 23145004
- PMCID: PMC3492249
- DOI: 10.1371/journal.pone.0048877
Clinical value of prognosis gene expression signatures in colorectal cancer: a systematic review
Abstract
Introduction: The traditional staging system is inadequate to identify those patients with stage II colorectal cancer (CRC) at high risk of recurrence or with stage III CRC at low risk. A number of gene expression signatures to predict CRC prognosis have been proposed, but none is routinely used in the clinic. The aim of this work was to assess the prediction ability and potential clinical usefulness of these signatures in a series of independent datasets.
Methods: A literature review identified 31 gene expression signatures that used gene expression data to predict prognosis in CRC tissue. The search was based on the PubMed database and was restricted to papers published from January 2004 to December 2011. Eleven CRC gene expression datasets with outcome information were identified and downloaded from public repositories. Random Forest classifier was used to build predictors from the gene lists. Matthews correlation coefficient was chosen as a measure of classification accuracy and its associated p-value was used to assess association with prognosis. For clinical usefulness evaluation, positive and negative post-tests probabilities were computed in stage II and III samples.
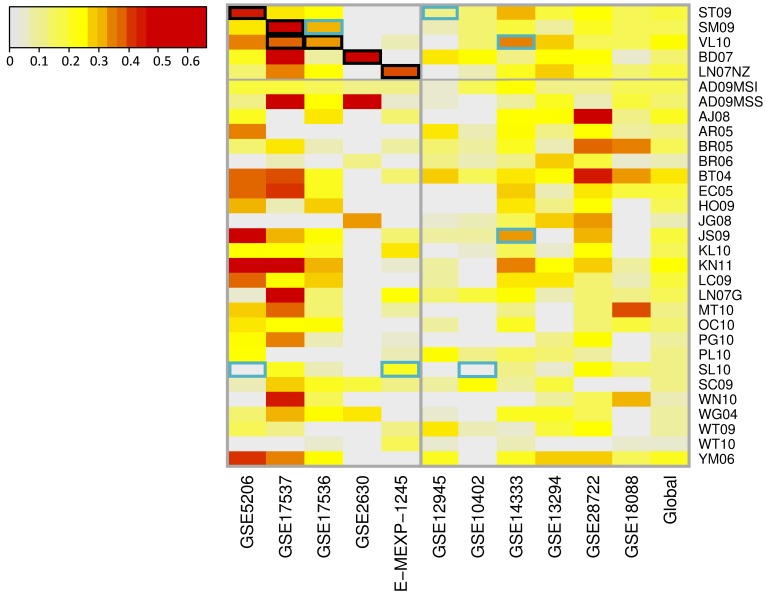
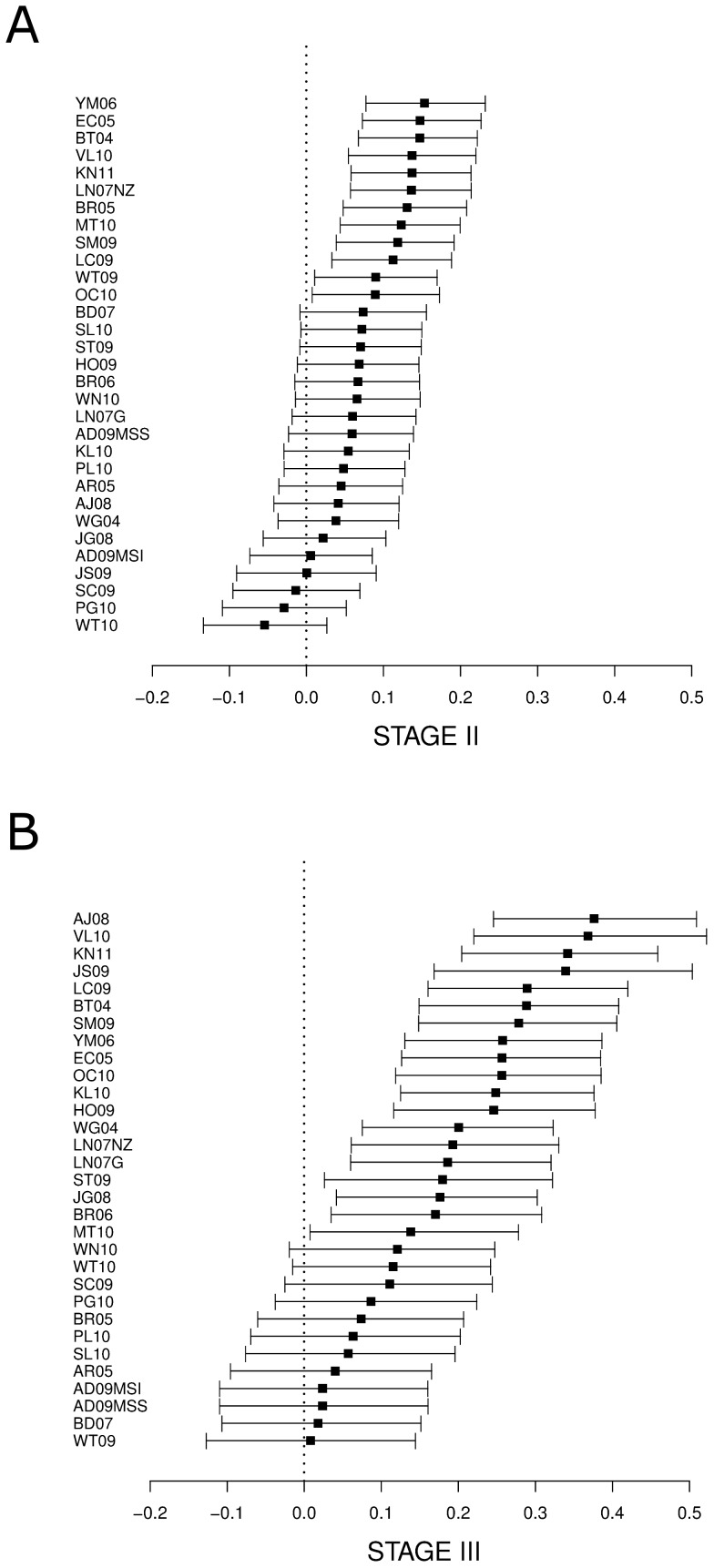
Results: Five gene signatures showed significant association with prognosis and provided reasonable prediction accuracy in their own training datasets. Nevertheless, all signatures showed low reproducibility in independent data. Stratified analyses by stage or microsatellite instability status showed significant association but limited discrimination ability, especially in stage II tumors. From a clinical perspective, the most predictive signatures showed a minor but significant improvement over the classical staging system.
Conclusions: The published signatures show low prediction accuracy but moderate clinical usefulness. Although gene expression data may inform prognosis, better strategies for signature validation are needed to encourage their widespread use in the clinic.
Conflict of interest statement
Figures

References
-
- Ferlay J, Parkin DM, Steliarova-Foucher E (2010) Estimates of cancer incidence and mortality in Europe in 2008. Eur J Cancer 46(4): 765–81. - PubMed
-
- Saltz LB, Kelsen DP (1997) Adjuvant treatment of colorectal cancer. Annu Rev Med 48: 191–202. - PubMed
-
- Benson AB 3rd, Schrag D, Somerfield MR, Cohen AM, Figueredo AT, et al (2004) American Society of Clinical Oncology recommendations on adjuvant chemotherapy for stage II colon cancer. J Clin Oncol 22(16): 3408–19. - PubMed
-
- Gill S, Loprinizi CL, Sargent DJ, Thome SD, Alberts SR, et al. (2004) Pooled analysis of fluorouracil-based adjuvant therapy for stage II and III colon cancer: who benefits and by how much?. J Clin Oncol 22(10): 1797–806. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
