

Diagnosing and staging of cystic echinococcosis: how do CT and MRI perform in comparison to ultrasound?
- PMID: 23145199
- PMCID: PMC3493391
- DOI: 10.1371/journal.pntd.0001880
Diagnosing and staging of cystic echinococcosis: how do CT and MRI perform in comparison to ultrasound?
Abstract
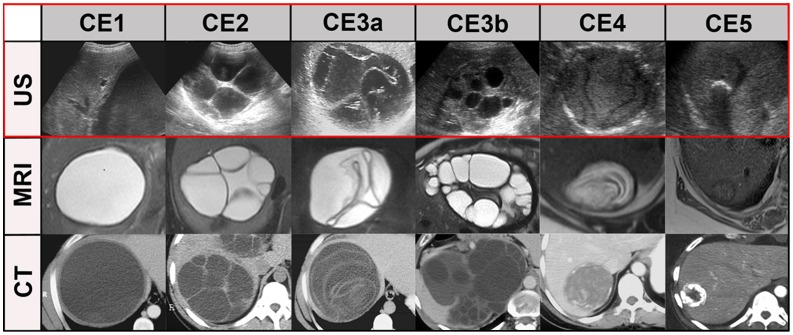
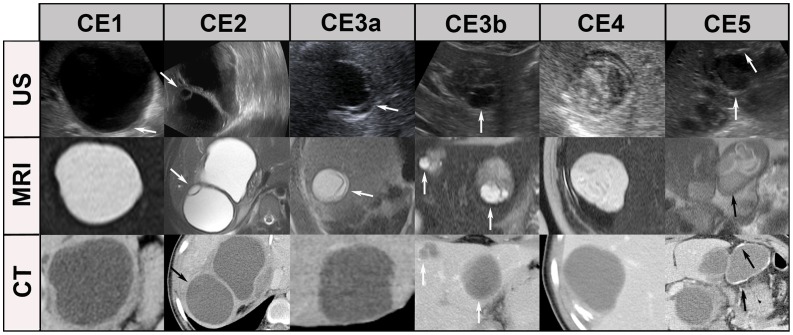
Background: Imaging plays the key role in diagnosing and staging of CE. The description of CE-specific imaging features and the WHO CE cyst classification is based on ultrasound. The reproducibility of the ultrasound-defined features of CE cysts is variable in MR- and CT-imaging. This is of particular importance for cysts that are not accessible by US and because of the increasing availability and overuse of CT and MR imaging.
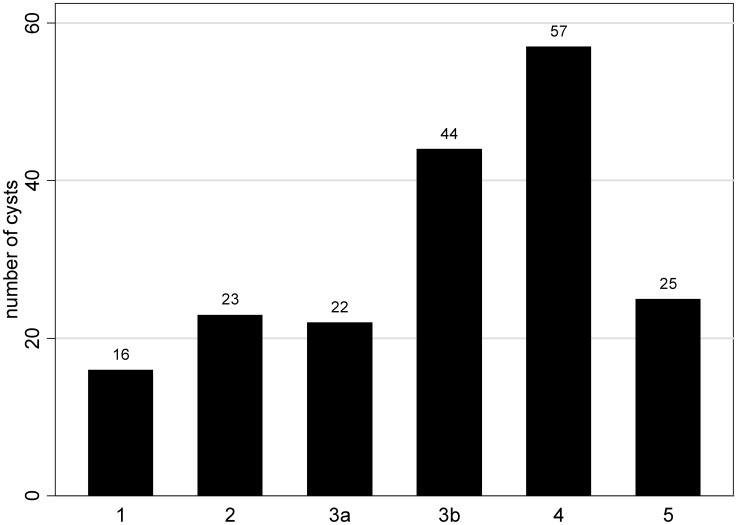
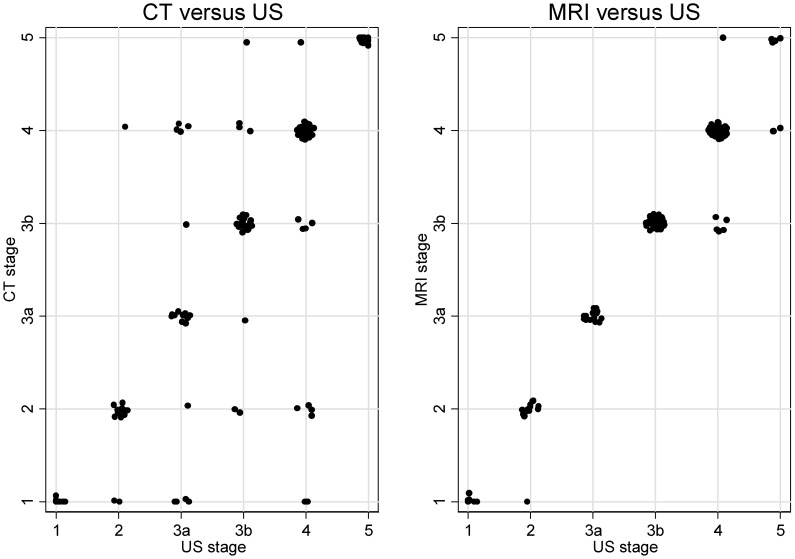
Methodology/principal findings: Retrospective analysis of patients with abdominal CE cysts of an interdisciplinary CE clinic who had CT and/or MRI scans performed additionally to US imaging. All images were read and interpreted by the same senior radiologist experienced in the diagnosis of CE. US, CT and MR images were staged according to the WHO classification criteria. The agreement beyond chance was quantified by kappa coefficients (κ). 107 patients with 187 CE cysts met the inclusion criteria. All cysts were assessed by US, 138 by CT, and 125 by MRI. The level of agreement beyond chance of the individual CE stages 1-4 was clearly lower for CT, with κ ranging from 0.62 to 0.72, compared to MRI with values of κ between 0.83 and 1.0. For CE5 cysts CT (κ = 0.95) performed better than MRI (κ = 0.65).
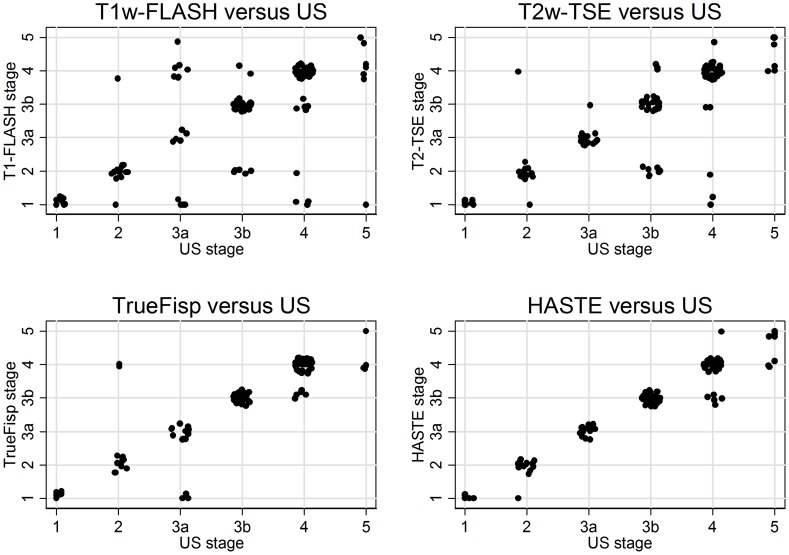
Conclusions: Ultrasound remains the corner stone of diagnosis, staging and follow up of CE cysts. MRI reproduces the ultrasound-defined features of CE better than CT. If US cannot be performed due to cyst location or patient-specific reasons MRI with heavily T2-weighted series is preferable to CT.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Craig PS, Larrieu E (2006) Control of cystic echinococcosis/hydatidosis: 1863–2002. Advances in Parasitology 61: 43–508. - PubMed
-
- Craig PS, McManus DP, Lightowlers MW, Chabalgoity JA, Garcia HH, et al. (2007) Prevention and control of cystic echinococcosis. Lancet Infect Dis 7: 385–394. - PubMed
-
- World Health Organization Informal Working Group (2003) International classification of ultrasound images in cystic echinococcosis for application in clinical and field epidemiological settings. Acta Trop 85: 253–261. - PubMed
-
- Gharbi HA, Hassine W, Brauner MW, Dupuch K (1981) Ultrasound examination of the hydatic liver. Radiology 139: 459–463. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
