

No serological evidence for a role of HHV-6 infection in chronic fatigue syndrome
- PMID: 23145212
- PMCID: PMC3493030
No serological evidence for a role of HHV-6 infection in chronic fatigue syndrome
Abstract
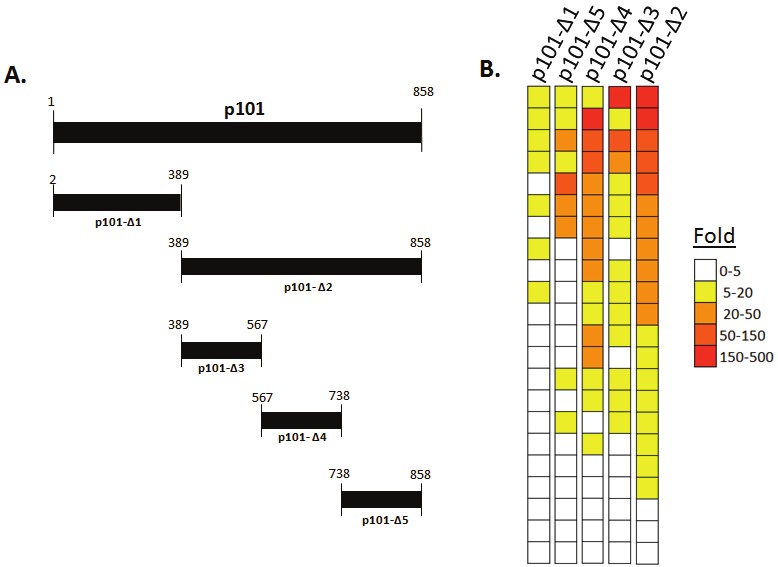
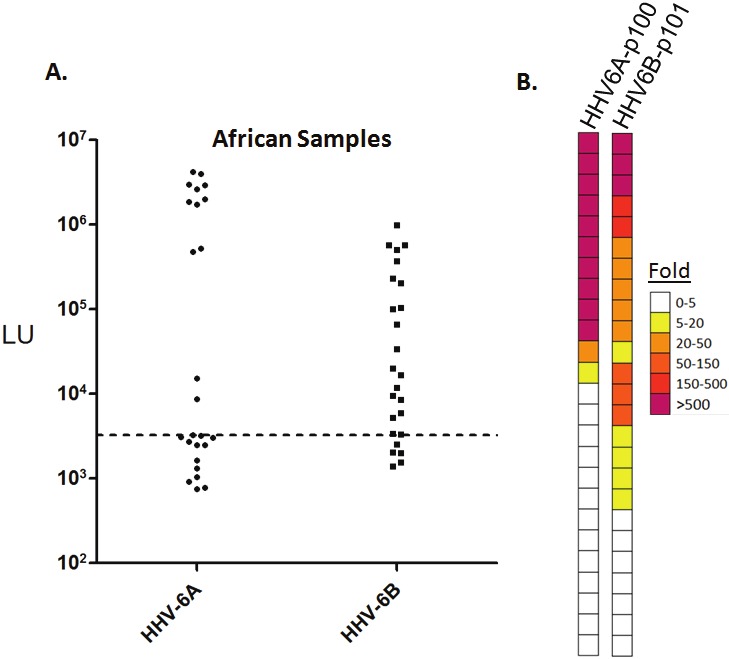
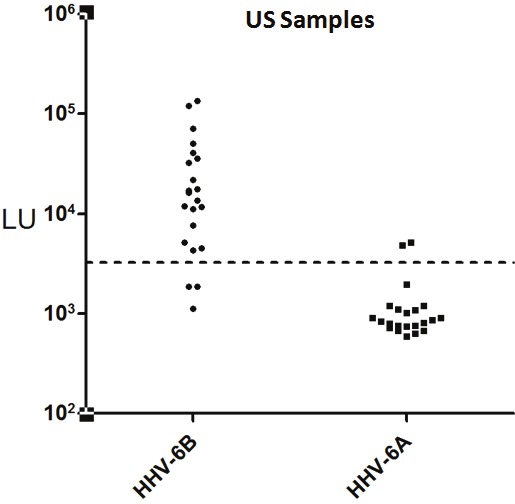
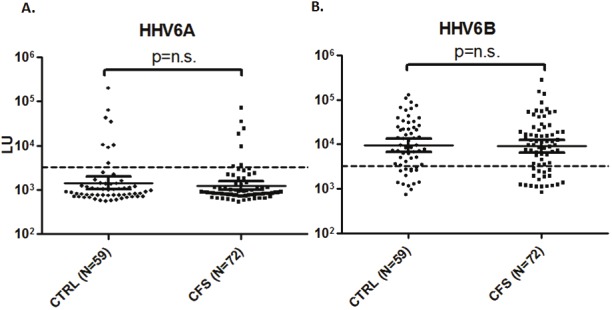
Human herpesvirus 6A (HHV-6A) and human herpesvirus 6B (HHV-6B) are associated with a variety of conditions including rash, fever, and encephalitis and may play a role in several neurological diseases. Here luciferase immunoprecipitation systems (LIPS) was used to develop HHV-6 serologic diagnostic tests using antigens encoded by the U11 gene from HHV-6A (p100) and HHV-6B (p101). Analysis of the antibody responses against Renilla luciferase fusions with different HHV-6B p101 fragments identified an antigenic fragment (amino acids 389 to 858) that demonstrated ~86% seropositivity in serum samples from healthy US blood donors. Additional experiments detected a HHV-6A antigenic fragment (amino acids 751-870) that showed ~48% antibody seropositivity in samples from Mali, Africa, a known HHV-6A endemic region. In contrast to the high levels of HHV-6A immunoreactivity seen in the African samples, testing of US blood donors with the HHV-6A p100 antigenic fragment revealed little immunoreactivity. To potentially explore the role of HHV-6 infection in human disease, a blinded cohort of controls (n=59) and chronic fatigue syndrome (CFS) patients (n=72) from the US was examined for serum antibodies. While only a few of the controls and CFS patients showed high level immunoreactivity with HHV-6A, a majority of both the controls and CFS patients showed significant immunoreactivity with HHV-6B. However, no statistically significant differences in antibody levels or frequency of HHV-6A or HHV-6B infection were detected between the controls and CFS patients. These findings highlight the utility of LIPS for exploring the seroepidemiology of HHV-6A and HHV-6B infection, but suggest that these viruses are unlikely to play a role in the pathogenesis of CFS.
Keywords: Chronic Fatigue Syndrome (CFS); Human Herpes Virus-6 (HHV6); luciferase immunoprecipitation systems (LIPS).
Figures
Similar articles
-
Antibodies to Human Herpesviruses in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Patients.Front Immunol. 2019 Aug 14;10:1946. doi: 10.3389/fimmu.2019.01946. eCollection 2019. Front Immunol. 2019. PMID: 31475007 Free PMC article.
-
The persistent viral infections in the development and severity of myalgic encephalomyelitis/chronic fatigue syndrome.J Transl Med. 2023 Jan 18;21(1):33. doi: 10.1186/s12967-023-03887-0. J Transl Med. 2023. PMID: 36653846 Free PMC article.
-
Inherited Chromosomally Integrated Human Herpesvirus 6 Demonstrates Tissue-Specific RNA Expression In Vivo That Correlates with an Increased Antibody Immune Response.J Virol. 2019 Dec 12;94(1):e01418-19. doi: 10.1128/JVI.01418-19. Print 2019 Dec 12. J Virol. 2019. PMID: 31597766 Free PMC article.
-
The role of herpesvirus 6A and 6B in multiple sclerosis and epilepsy.Scand J Immunol. 2020 Dec;92(6):e12984. doi: 10.1111/sji.12984. Epub 2020 Oct 23. Scand J Immunol. 2020. PMID: 33037649 Free PMC article. Review.
-
Update on infections with human herpesviruses 6A, 6B, and 7.Med Mal Infect. 2017 Mar;47(2):83-91. doi: 10.1016/j.medmal.2016.09.004. Epub 2016 Oct 20. Med Mal Infect. 2017. PMID: 27773488 Review.
Cited by
-
Human herpes simplex virus-6 (HHV-6) detection and seroprevalence among Qatari nationals and immigrants residing in Qatar.IJID Reg. 2021 Dec 16;2:90-95. doi: 10.1016/j.ijregi.2021.12.005. eCollection 2022 Mar. IJID Reg. 2021. PMID: 35757074 Free PMC article.
-
Classification of HHV-6A and HHV-6B as distinct viruses.Arch Virol. 2014 May;159(5):863-70. doi: 10.1007/s00705-013-1902-5. Epub 2013 Nov 6. Arch Virol. 2014. PMID: 24193951 Free PMC article. Review.
-
Herpesviruses dUTPases: A New Family of Pathogen-Associated Molecular Pattern (PAMP) Proteins with Implications for Human Disease.Pathogens. 2016 Dec 28;6(1):2. doi: 10.3390/pathogens6010002. Pathogens. 2016. PMID: 28036046 Free PMC article. Review.
-
Human Herpesvirus 6 Infection and Risk of Chronic Fatigue Syndrome: A Systematic Review and Meta-Analysis.Intervirology. 2022;65(1):49-57. doi: 10.1159/000517930. Epub 2021 Jun 23. Intervirology. 2022. PMID: 34348314 Free PMC article.
-
Deficient EBV-specific B- and T-cell response in patients with chronic fatigue syndrome.PLoS One. 2014 Jan 15;9(1):e85387. doi: 10.1371/journal.pone.0085387. eCollection 2014. PLoS One. 2014. PMID: 24454857 Free PMC article.
References
-
- Tanaka-Taya K, Kondo T, Mukai T, Miyoshi H, Yamamoto Y, Okada S, Yamanishi K. Seroepidemiological study of human herpesvirus-6 and -7 in children of different ages and detection of these two viruses in throat swabs by polymerase chain reaction. J Med Virol. 1996;48:88–94. - PubMed
-
- Boutolleau D, Duros C, Bonnafous P, Caiola D, Karras A, Castro ND, Ouachee M, Narcy P, Gueudin M, Agut H, Gautheret-Dejean A. Identification of human herpesvirus 6 variants A and B by primer-specific real-time PCR may help to revisit their respective role in pathology. J Clin Virol. 2006;35:257–263. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources