

Human rhinovirus C: Age, season, and lower respiratory illness over the past 3 decades
- PMID: 23146382
- PMCID: PMC3748586
- DOI: 10.1016/j.jaci.2012.09.033
Human rhinovirus C: Age, season, and lower respiratory illness over the past 3 decades
Abstract
Background: Human rhinoviruses (HRVs) cause common colds, and the recently discovered HRV-C is increasingly associated with lower respiratory illness among populations such as children and asthmatic patients.
Objective: To determine how HRV-C is associated with respiratory illness and to evaluate changes in prevalence and species over 2 decades.
Methods: A prospective study of children younger than 5 years was performed at the Vanderbilt Vaccine Clinic over a 21-year period. Nasal-wash specimens from children presenting with upper or lower respiratory illness at acute care visits were tested for HRV and HRV-positives genotyped. Demographic and clinical features were compared between children with or without HRV, and with different HRV species.
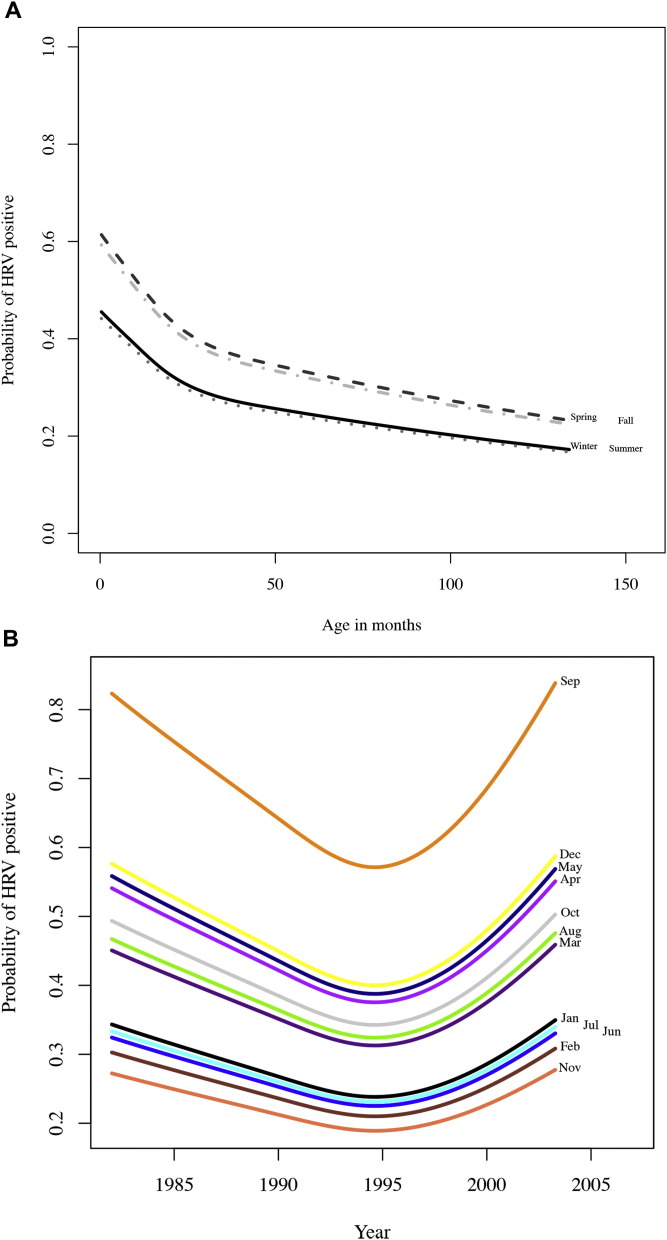
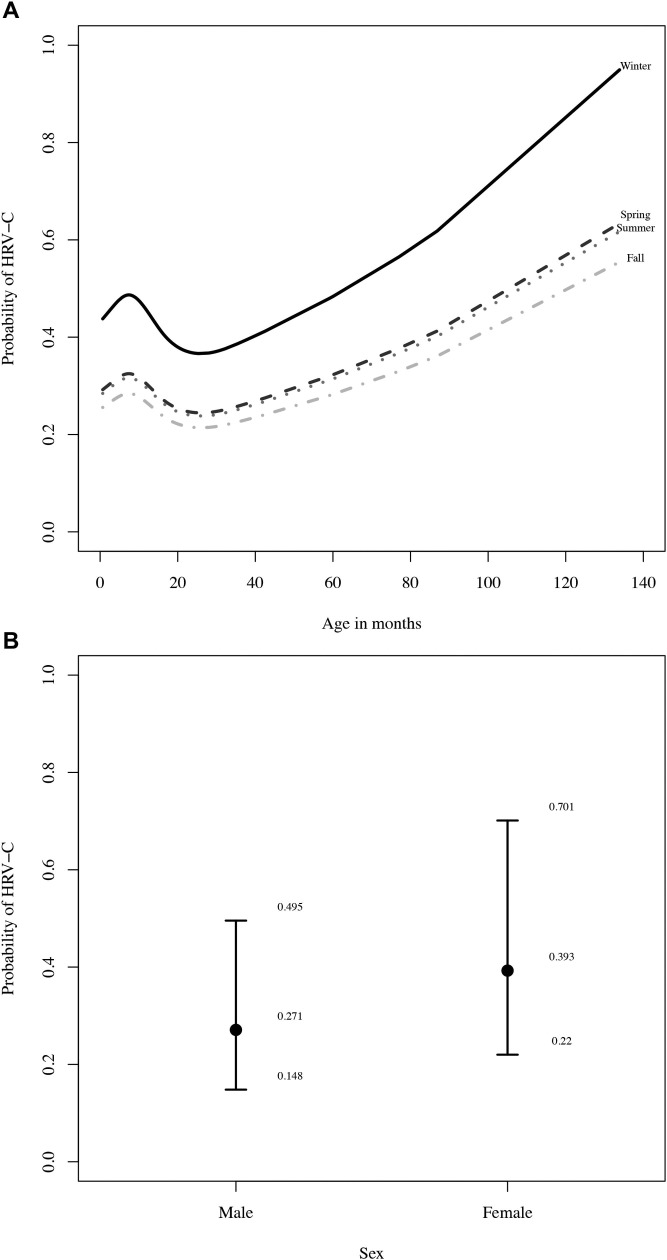
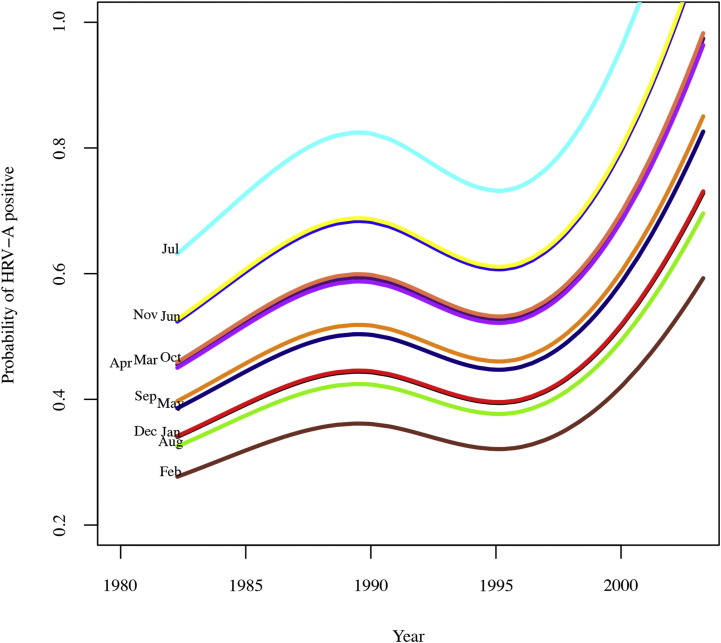
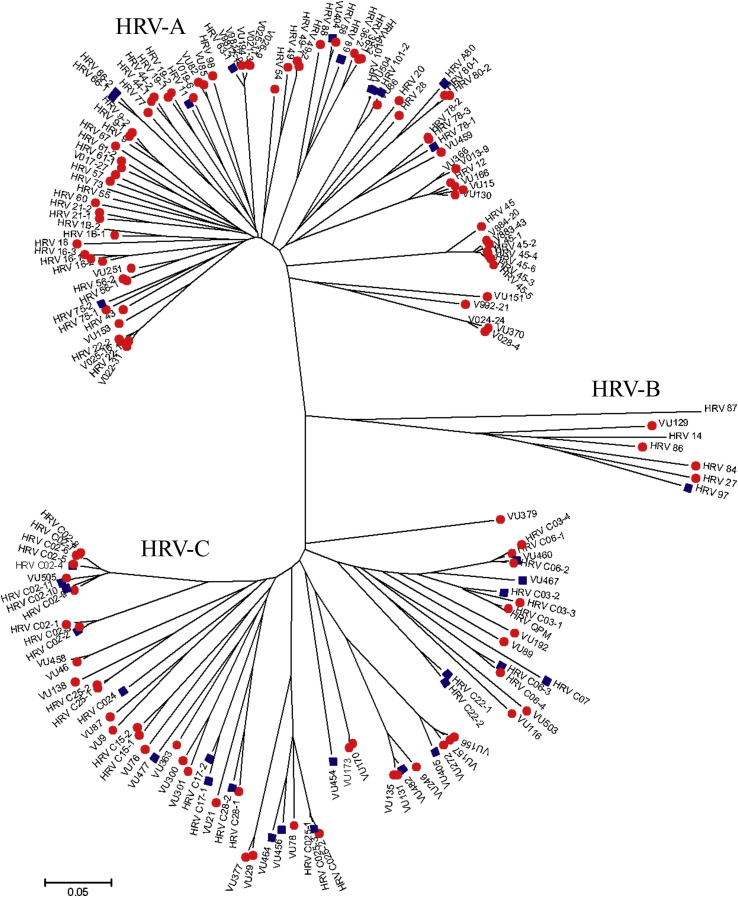
Results: HRV was detected in 190 of 527 (36%) specimens from a population of 2009 children from 1982 through 2003. Of these, 36% were HRV-C. Age (P = .039) and month of illness (P < .001) were associated with HRV infection and HRV species. HRV-C was significantly associated with lower respiratory illness, compared with HRV-A (P = .014). HRV-A and HRV-C prevalence fluctuated throughout the 21-year period; HRV-C was more prevalent during winter (P = .058).
Conclusions: HRV-C is not a new virus but has been significantly associated with childhood lower respiratory illness in this population for several decades. Temporal changes in virus prevalence occur, and season may predict virus species. Our findings have implications for diagnostic, preventive, and treatment strategies due to the variation in disease season and severity based on species of HRV infection.
Copyright © 2012 American Academy of Allergy, Asthma & Immunology. Published by Mosby, Inc. All rights reserved.
Figures



References
-
- Pelon W., Mogabgab W., Phillips I., Pierce W. A cytopathogenic agent isolated from naval recruits with mild respiratory illnesses. Proc Soc Exp Biol Med. 1957;94:262–267. - PubMed
-
- Hamparian V.V. A collaborative report—rhinoviruses, extensions of the numbering system from 89 to 100. Virology. 1987;159:191–192. - PubMed
-
- Simmonds P., McIntyre C., Savolainen-Kopra C., Tapparel C., Mackay I.M., Hovi T. Proposals for the classification of human rhinovirus species C into genotypically assigned types. J Gen Virol. 2010;91:2409–2419. - PubMed
-
- Louie J.K., Roy-Burman A., Guardia-LaBar L., Boston E.J., Kiang D., Padilla T. Rhinovirus associated with severe lower respiratory tract infections in children. Pediatr Infect Dis J. 2009;28:337–339. - PubMed
Publication types
MeSH terms
Associated data
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
